

Mechanical circulatory support in patients with cardiogenic shock not secondary to cardiotomy: a network meta-analysis
- PMID: 33677732
- PMCID: PMC9033692
- DOI: 10.1007/s10741-021-10092-y
Mechanical circulatory support in patients with cardiogenic shock not secondary to cardiotomy: a network meta-analysis
Abstract
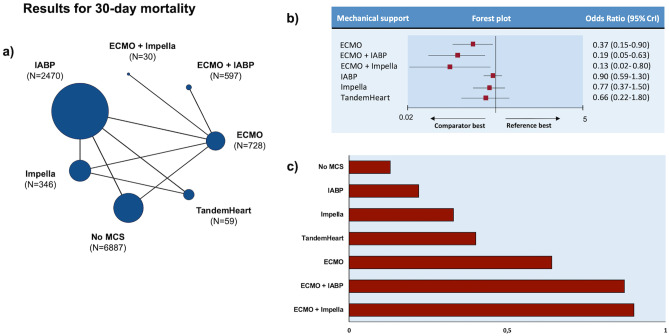
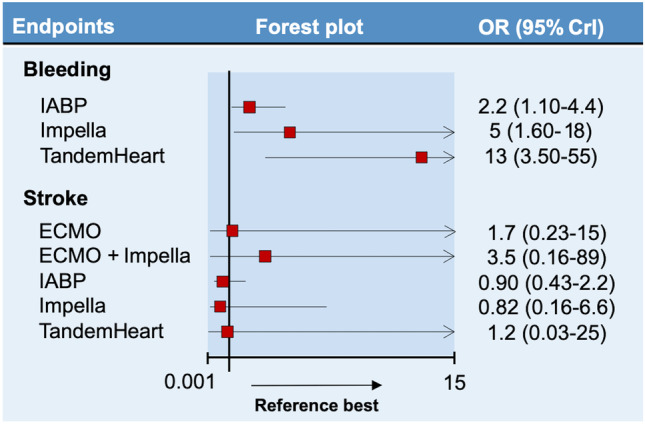
To compare the efficacy and safety of different mechanical circulatory support (MCS) devices in CS. A total of 24 studies (7 randomized controlled trials-RCTs-and 17 non-RCTs) involving 11,117 patients were entered in a Bayesian network meta-analysis. The primary endpoint was 30-day mortality. Secondary endpoints were stroke and bleeding (requiring transfusion and/or intracranial and/or fatal). Compared with no MCS, extra-corporeal membrane oxygenation (ECMO) reduced 30-day mortality when used both alone (OR 0.37, 95% CrI 0.15-0.90) and together with the micro-axial pump Impella (OR 0.13, 95% CrI 0.02-0.80) or intra-aortic balloon pump (IABP) (OR 0.19, 95% CrI 0.05-0.63), although the relevant articles were affected by significant publication bias. Consistent results were obtained in a sensitivity analysis including only studies of CS due to myocardial infarction. After halving the weight of studies with a non-RCT design, only the benefit of ECMO + IABP on 30-day mortality was maintained (OR 0.22, 95% CI 0.057-0.76). The risk of bleeding was increased by TandemHeart (OR 13, 95% CrI 3.50-59), Impella (OR 5, 95% CrI 1.60-18), and IABP (OR 2.2, 95% CrI 1.10-4.4). No significant differences were found across MCS strategies regarding stroke. Although limited by important quality issues, the studies performed so far indicate that ECMO, especially if combined with Impella or IABP, reduces short-term mortality in CS. MCS increases the hazard of bleeding.
Keywords: Cardiogenic shock; Extracorporeal membrane oxygenation; Impella; Intra-aortic balloon pump; Mechanical circulatory support; TandemHeart.
© 2021. The Author(s).
Conflict of interest statement
Dr. Ameri reports personal fees from Novartis, personal fees from Astra Zeneca, personal fees from Vifor, personal fees from Daiichi-Sankyo, personal fees from Boehringer Ingelheim, personal fees from Janssen, personal fees from Merck Sharp & Dohme, and personal fees from GlaxoSmithKline, outside the submitted work; Dr. Porto reports grants and personal fees from AstraZeneca, personal fees from Daiichi Sankyo, personal fees from Terumo Corporation, personal fees from Biotronik, personal fees from Bayer, personal fees from Amgen, and personal fees and non-financial support from Abiomed, outside the submitted work; Dr. Canepa reports grants and personal fees from Pfizer, personal fees from Novartis, personal fees from Akcea Therapeutics, and personal fees from Sanofi Genzyme, outside the submitted work; Dr. Crimi reports personal fees from Philips healthcare, outside the submitted work; other authors have nothing to disclose.
Figures
References
-
- Lauridsen MD, Rørth R, Lindholm MG, et al. Trends in first-time hospitalization, management, and short-term mortality in acute myocardial infarction–related cardiogenic shock from 2005 to 2017: a nationwide cohort study. Am Heart J. 2020;28(229):127–137. doi: 10.1016/j.ahj.2020.08.012. - DOI - PubMed
-
- van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136(16):e232–e268. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG et al (1999) Early revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med 341(9):625–34 - PubMed
-
- O’Connor CM, Gattis WA, Uretsky BF, et al. Continuous intravenous dobutamine is associated with an increased risk of death in patients with advanced heart failure: Insights from the Flolan International Randomized Survival Trial (FIRST) Am Heart J. 1999;138(1 Pt 1):78–86. doi: 10.1016/S0002-8703(99)70250-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
