The Genotype-Based Morphology of Aldosterone-Producing Adrenocortical Disorders and Their Association with Aging
- PMID: 33677921
- PMCID: PMC7937858
- DOI: 10.3803/EnM.2021.101
The Genotype-Based Morphology of Aldosterone-Producing Adrenocortical Disorders and Their Association with Aging
Abstract
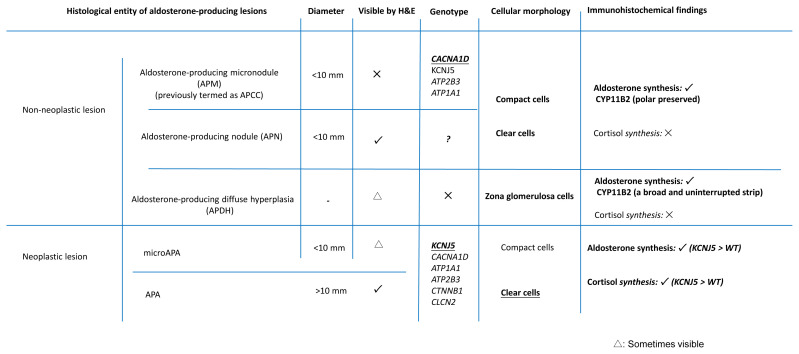
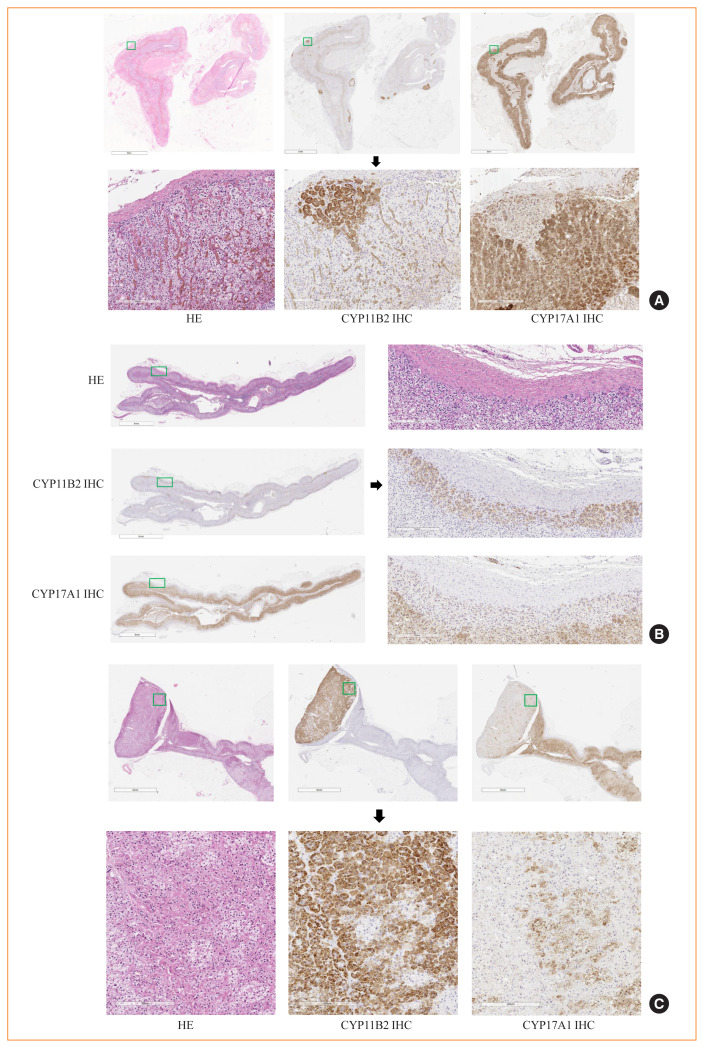
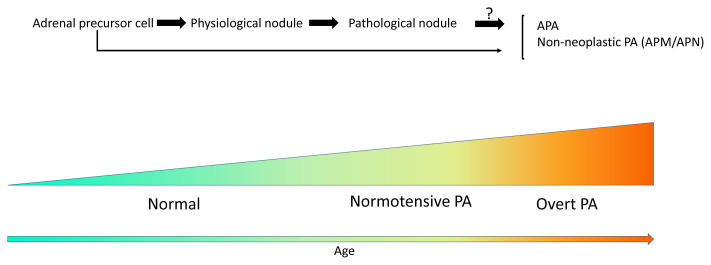
Primary aldosteronism (PA) is the most common cause of secondary hypertension, and is associated with an increased incidence of cardiovascular events. PA itself is clinically classified into the following two types: unilateral PA, mostly composed of aldosteroneproducing adenoma (APA); and bilateral hyperaldosteronism, consisting of multiple aldosterone-producing micronodules (APMs) and aldosterone-producing diffuse hyperplasia. Histopathologically, those disorders above are all composed of compact and clear cells. The cellular morphology in the above-mentioned aldosterone-producing disorders has been recently reported to be closely correlated with patterns of somatic mutations of ion channels including KCNJ5, CACNA1D, ATP1A1, ATP2B3, and others. In addition, in non-pathological adrenal glands, APMs are frequently detected regardless of the status of the renin-angiotensin-aldosterone system (RAAS). Aldosterone-producing nodules have been also proposed as non-neoplastic nodules that can be identified by hematoxylin and eosin staining. These non-neoplastic CYP11B2-positive nodules could represent possible precursors of APAs possibly due to the presence of somatic mutations. On the other hand, aging itself also plays a pivotal role in the development of aldosterone-producing lesions. For instance, the number of APMs was also reported to increase with aging. Therefore, recent studies indicated the novel classification of PA into normotensive PA (RAAS-independent APM) and clinically overt PA.
Keywords: Adenoma; Adrenal glands; Aldosterone; Pathology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
Clinical Translationality of KCNJ5 Mutation in Aldosterone Producing Adenoma.Int J Mol Sci. 2022 Aug 12;23(16):9042. doi: 10.3390/ijms23169042. Int J Mol Sci. 2022. PMID: 36012306 Free PMC article. Review.
-
Immunohistochemical, genetic and clinical characterization of sporadic aldosterone-producing adenomas.Mol Cell Endocrinol. 2015 Aug 15;411:146-54. doi: 10.1016/j.mce.2015.04.022. Epub 2015 May 6. Mol Cell Endocrinol. 2015. PMID: 25958045 Free PMC article.
-
Pathology of Aldosterone Biosynthesis and its Action.Tohoku J Exp Med. 2021 May;254(1):1-15. doi: 10.1620/tjem.254.1. Tohoku J Exp Med. 2021. PMID: 34011803
-
Histological Characterization of Aldosterone-producing Adrenocortical Adenomas with Different Somatic Mutations.J Clin Endocrinol Metab. 2020 Mar 1;105(3):e282-9. doi: 10.1210/clinem/dgz235. J Clin Endocrinol Metab. 2020. PMID: 31789380 Free PMC article.
-
Histopathological features of aldosterone-producing lesions according to their different somatic genetic mutations.Vitam Horm. 2025;129:125-141. doi: 10.1016/bs.vh.2024.09.001. Epub 2024 Oct 15. Vitam Horm. 2025. PMID: 40812944 Review.
Cited by
-
Cellular Senescence in Adrenocortical Biology and Its Disorders.Cells. 2021 Dec 9;10(12):3474. doi: 10.3390/cells10123474. Cells. 2021. PMID: 34943980 Free PMC article. Review.
-
2023 Korean Endocrine Society Consensus Guidelines for the Diagnosis and Management of Primary Aldosteronism.Endocrinol Metab (Seoul). 2023 Dec;38(6):597-618. doi: 10.3803/EnM.2023.1789. Epub 2023 Oct 13. Endocrinol Metab (Seoul). 2023. PMID: 37828708 Free PMC article.
References
-
- Funder JW. Medicine: the genetics of primary aldosteronism. Science. 2011;331:685–6. - PubMed
-
- Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C, et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol. 2006;48:2293–300. - PubMed
-
- Williams JS, Williams GH, Raji A, Jeunemaitre X, Brown NJ, Hopkins PN, et al. Prevalence of primary hyperaldosteronism in mild to moderate hypertension without hypokalaemia. J Hum Hypertens. 2006;20:129–36. - PubMed
-
- Nishimoto K, Nakagawa K, Li D, Kosaka T, Oya M, Mikami S, et al. Adrenocortical zonation in humans under normal and pathological conditions. J Clin Endocrinol Metab. 2010;95:2296–305. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources