

Association Between Increased Hospital Reimbursement for Cardiac Rehabilitation and Utilization of Cardiac Rehabilitation by Medicare Beneficiaries: An Interrupted Time Series
- PMID: 33677975
- PMCID: PMC8035974
- DOI: 10.1161/CIRCOUTCOMES.120.006572
Association Between Increased Hospital Reimbursement for Cardiac Rehabilitation and Utilization of Cardiac Rehabilitation by Medicare Beneficiaries: An Interrupted Time Series
Abstract
Background: Although cardiac rehabilitation (CR) is a Class I Guideline recommendation, and has been shown to be a cost-effective intervention after a cardiac event, it has been reimbursed at levels insufficient to cover hospital operating costs. In January 2011, Medicare increased payment for CR in hospital outpatient settings by ≈180%. We evaluated the association between this payment increase and participation in CR of eligible Medicare beneficiaries to better understand the relationship between reimbursement policy and CR utilization.
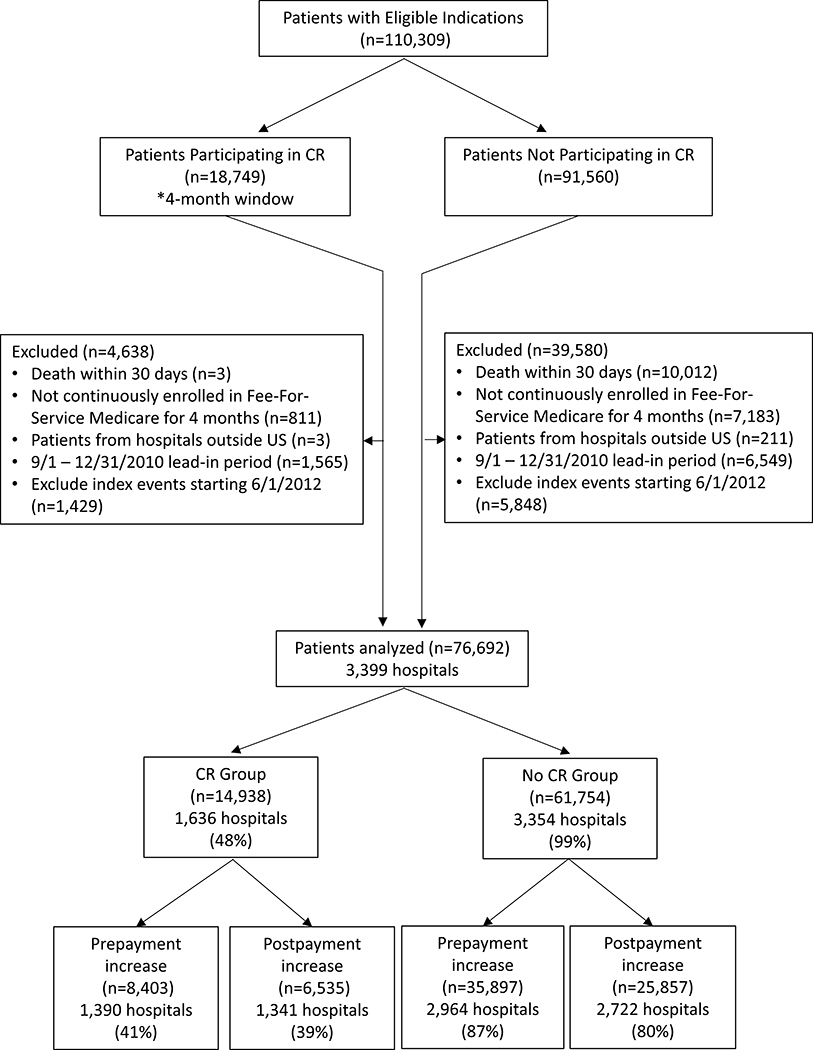
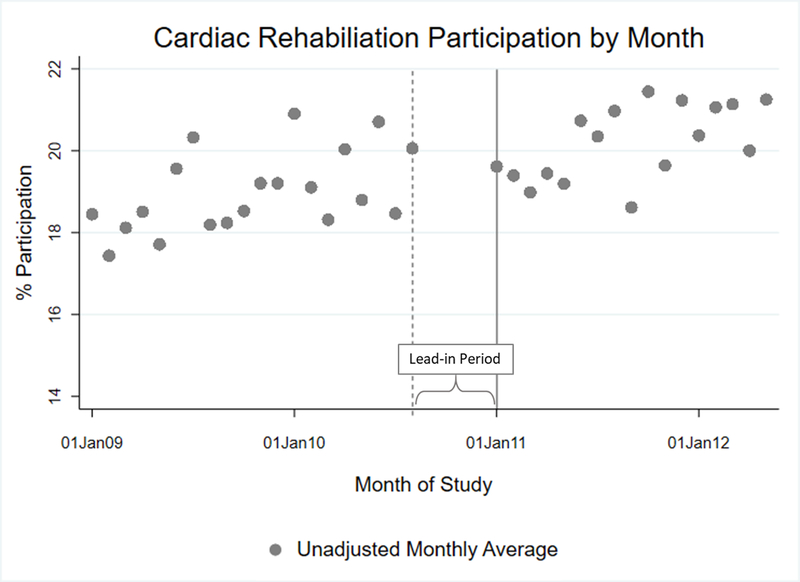
Methods: From a 5% Medicare claims sample, we identified patients with acute myocardial infarction, coronary artery bypass surgery, percutaneous coronary intervention, or cardiac valve surgery between January 1, 2009 and September 30, 2012, alive 30 days after their event, with continuous enrollment in Medicare fee-for-service, Part A/B for 4 months. Trends and changes in CR participation were estimated using an interrupted time series approach with a hierarchical logistic model, hospital random intercepts, adjusted for patient, hospital, market, and seasonality factors. Estimates were expressed using average marginal effects on a percent scale.
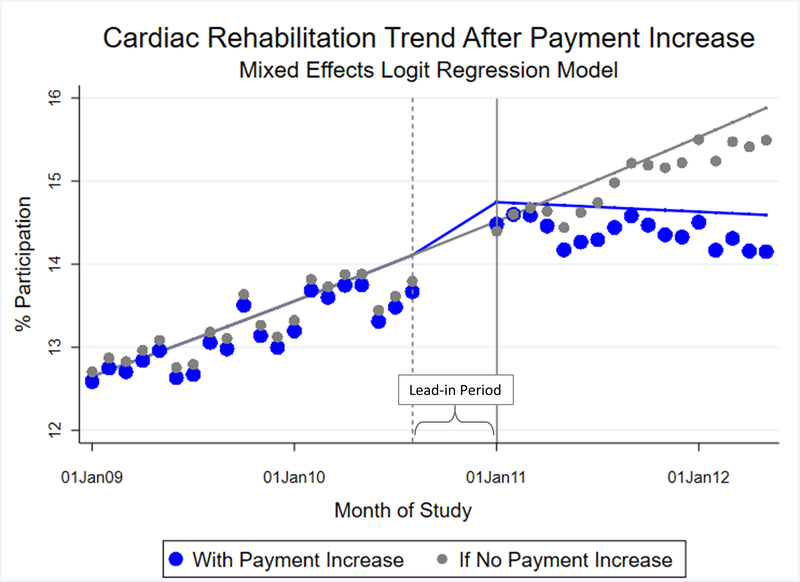
Results: Among 76 695 eligible patients, average annual CR participation was 19.5% overall. In the period before payment increase, adjusted annual participation grew by 1.1 percentage points (95% CI, 0.48-2.4). No immediate change occurred in CR participation when the new payment was implemented. In the period after payment increase, on average, 20% of patients participated in CR annually. The annual growth rate in CR participation slowed in the post-period by 1.3 percentage points (95% CI, -2.4 to -0.12) compared with the prior period. Results were somewhat sensitive to time window variations.
Conclusions: The 2011 increase in Medicare reimbursement for CR was not associated with an increase in participation. Future studies should evaluate whether payment did not reach a threshold to incentivize hospitals or if hospitals were not sensitive to reimbursement changes.
Keywords: cardiac rehabilitation; hospital; myocardial infarction; outpatient; percutaneous coronary intervention.
Figures
Similar articles
-
Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative.Circ Cardiovasc Qual Outcomes. 2020 Jan;13(1):e005902. doi: 10.1161/CIRCOUTCOMES.119.005902. Epub 2020 Jan 14. Circ Cardiovasc Qual Outcomes. 2020. PMID: 31931615 Free PMC article.
-
Health Care Use and Expenditures Associated With Cardiac Rehabilitation Among Eligible Medicare Fee-for-Service Beneficiaries.J Am Heart Assoc. 2025 Mar 4;14(5):e037811. doi: 10.1161/JAHA.124.037811. Epub 2025 Feb 24. J Am Heart Assoc. 2025. PMID: 39989369 Free PMC article.
-
Hospital-level variation in cardiac rehabilitation metrics.Am Heart J. 2025 Apr;282:58-69. doi: 10.1016/j.ahj.2024.12.004. Epub 2024 Dec 13. Am Heart J. 2025. PMID: 39675500
-
Payment methods for healthcare providers working in outpatient healthcare settings.Cochrane Database Syst Rev. 2021 Jan 20;1(1):CD011865. doi: 10.1002/14651858.CD011865.pub2. Cochrane Database Syst Rev. 2021. PMID: 33469932 Free PMC article.
-
Barriers to Participation in Cardiac Rehabilitation Among Patients with Coronary Heart Disease After Reperfusion Therapy: A Scoping Review.Vasc Health Risk Manag. 2023 Aug 31;19:557-570. doi: 10.2147/VHRM.S425505. eCollection 2023. Vasc Health Risk Manag. 2023. PMID: 37671387 Free PMC article.
Cited by
-
Applying User-Centered Design and Implementation Science to the Early-Stage Development of a Telehealth-Enhanced Hybrid Cardiac Rehabilitation Program: Quality Improvement Study.JMIR Form Res. 2023 Jul 13;7:e47264. doi: 10.2196/47264. JMIR Form Res. 2023. PMID: 37440285 Free PMC article.
-
Clin-STAR Corner: Rehabilitation for Older Adults With Heart Failure.J Am Geriatr Soc. 2025 Jun;73(6):1697-1703. doi: 10.1111/jgs.19346. Epub 2025 Jan 26. J Am Geriatr Soc. 2025. PMID: 39865546 Review.
-
Cardiac Rehabilitation in the Modern Era: Evidence, Equity, and Evolving Delivery Models Across the Cardiovascular Spectrum.J Clin Med. 2025 Aug 7;14(15):5573. doi: 10.3390/jcm14155573. J Clin Med. 2025. PMID: 40807202 Free PMC article. Review.
-
User-centered design of a telehealth-enhanced hybrid cardiac rehabilitation program as hospital quality improvement.Res Sq [Preprint]. 2023 Jan 16:rs.3.rs-2475875. doi: 10.21203/rs.3.rs-2475875/v1. Res Sq. 2023. Update in: JMIR Form Res. 2023 Jul 13;7:e47264. doi: 10.2196/47264. PMID: 36711987 Free PMC article. Updated. Preprint.
References
-
- United States Department of Health and Human Services. The Centers for Medicare and Medicaid Services. Decision Memo For Cardiac Rehabilitation (CR) Programs - Chronic Heart Failure (CAG-00437N) [Internet]. 2014. [Accessed February 01, 2019]. Available from: https://www.cms.gov/medicare-coverage-database/details/nca-decision-memo...
-
- Thomas RJ, Balady G, Banka G, Beckie TM, Chiu J, Gokak S, Ho PM, Keteyian SJ, King M, Lui K, Pack Q, Sanderson BK, Wang TY. 2018 ACC/AHA clinical performance and quality measures for cardiac rehabilitation: A report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. Circ Cardiovasc Qual Outcomes. 2018;11:1–29. - PubMed
-
- Leggett LE, Hauer T, Martin BJ, Manns B, Aggarwal S, Arena R, Austford LD, Meldrum D, Ghali W, Knudtson ML, Norris CM, Stone JA, Clement F. Optimizing Value From Cardiac Rehabilitation: A Cost-Utility Analysis Comparing Age, Sex, and Clinical Subgroups. Mayo Clin Proc. 2015;90:1011–1020. - PubMed
-
- Lee AJ, Shepard DS. Costs of Cardiac Rehabilitation and Enhanced Lifestyle Modification Programs. J Cardiopulm Rehabil Prev. 2009;29:348–357. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
