

Development of a novel, sensitive translational immunoassay to detect plasma glial fibrillary acidic protein (GFAP) after murine traumatic brain injury
- PMID: 33678186
- PMCID: PMC7938597
- DOI: 10.1186/s13195-021-00793-9
Development of a novel, sensitive translational immunoassay to detect plasma glial fibrillary acidic protein (GFAP) after murine traumatic brain injury
Abstract
Background: Glial fibrillary acidic protein (GFAP) has emerged as a promising fluid biomarker for several neurological indications including traumatic brain injury (TBI), a leading cause of death and disability worldwide. In humans, serum or plasma GFAP levels can predict brain abnormalities including hemorrhage on computed tomography (CT) scans and magnetic resonance imaging (MRI). However, assays to quantify plasma or serum GFAP in preclinical models are not yet available.
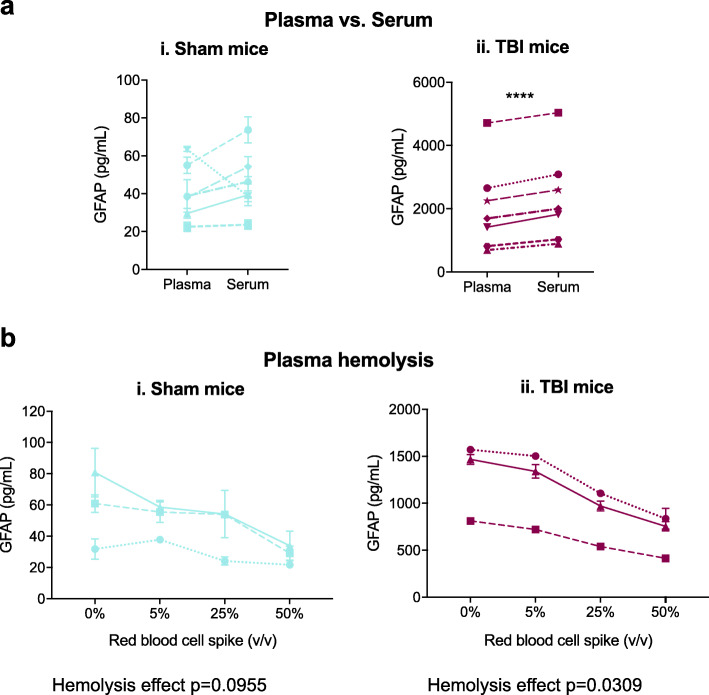
Methods: We developed and validated a novel sensitive GFAP immunoassay assay for mouse plasma on the Meso Scale Discovery immunoassay platform and validated assay performance for robustness, precision, limits of quantification, dilutional linearity, parallelism, recovery, stability, selectivity, and pre-analytical factors. To provide proof-of-concept data for this assay as a translational research tool for TBI and Alzheimer's disease (AD), plasma GFAP was measured in mice exposed to TBI using the Closed Head Impact Model of Engineered Rotational Acceleration (CHIMERA) model and in APP/PS1 mice with normal or reduced levels of plasma high-density lipoprotein (HDL).
Results: We performed a partial validation of our novel assay and found its performance by the parameters studied was similar to assays used to quantify human GFAP in clinical neurotrauma blood specimens and to assays used to measure murine GFAP in tissues. Specifically, we demonstrated an intra-assay CV of 5.0%, an inter-assay CV of 7.2%, a lower limit of detection (LLOD) of 9.0 pg/mL, a lower limit of quantification (LLOQ) of 24.8 pg/mL, an upper limit of quantification (ULOQ) of at least 16,533.9 pg/mL, dilution linearity of calibrators from 20 to 200,000 pg/mL with 90-123% recovery, dilution linearity of plasma specimens up to 32-fold with 96-112% recovery, spike recovery of 67-100%, and excellent analyte stability in specimens exposed to up to 7 freeze-thaw cycles, 168 h at 4 °C, 24 h at room temperature (RT), or 30 days at - 20 °C. We also observed elevated plasma GFAP in mice 6 h after TBI and in aged APP/PS1 mice with plasma HDL deficiency. This assay also detects GFAP in serum.
Conclusions: This novel assay is a valuable translational tool that may help to provide insights into the mechanistic pathophysiology of TBI and AD.
Keywords: CHIMERA; GFAP; Immunoassay; Plasma biomarker; TBI.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures









References
-
- FDA authorizes marketing of first blood test to aid in the evaluation of concussion in adults. 2018. Available from: https://www.fda.gov/news-events/press-announcements/fda-authorizes-marke.... Accessed 18 Sep 2020.
-
- Anderson TN, Hwang J, Munar M, Papa L, Hinson HE, Vaughan A, et al. Blood-based biomarkers for prediction of intracranial hemorrhage and outcome in patients with moderate or severe traumatic brain injury. J Trauma Acute Care Surg. 2020;89(1):80–86. doi: 10.1097/TA.0000000000002706. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
