

Association of frequent moisturizer use in early infancy with the development of food allergy
- PMID: 33678253
- PMCID: PMC9393761
- DOI: 10.1016/j.jaci.2020.10.044
Association of frequent moisturizer use in early infancy with the development of food allergy
Abstract
Background: Food allergy is thought to develop through transcutaneous sensitization, especially in the presence of skin barrier impairment and inflammation. Regular moisturizer application to infant skin could potentially promote transcutaneous sensitization and the development of food allergy.
Objectives: We tested this hypothesis in the Enquiring About Tolerance (EAT) study population.
Methods: The EAT study was a population-based randomized clinical trial conducted from January 15, 2008, to August 31, 2015, and recruited 1303 exclusively breastfed 3-month-old infants and their families from England and Wales. At enrollment at 3 months, families completed a questionnaire that included questions about frequency and type of moisturizer applied, use of corticosteroid creams, and parental report of dry skin or eczema. Infants were examined for visible eczema at the enrollment visit.
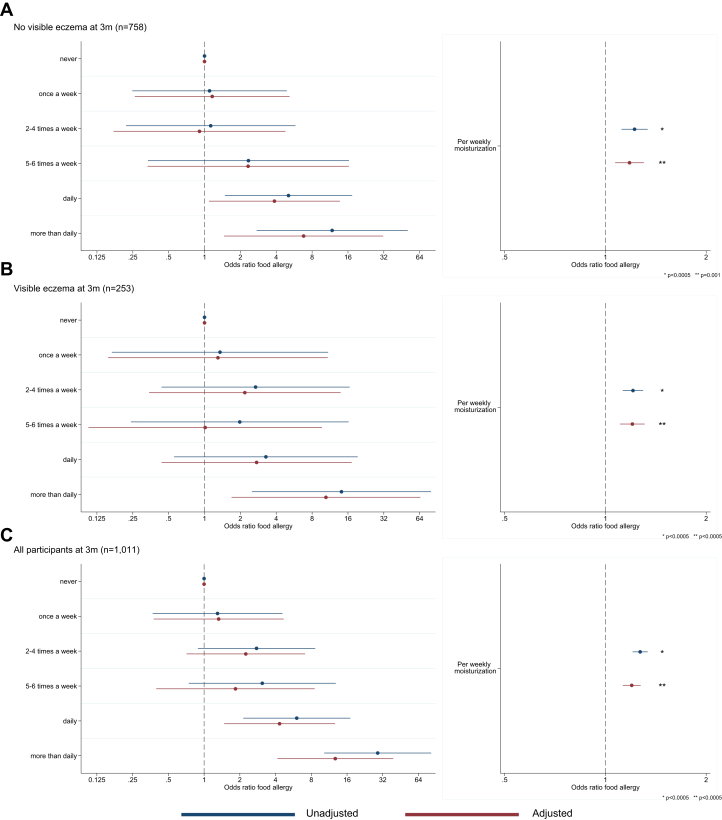
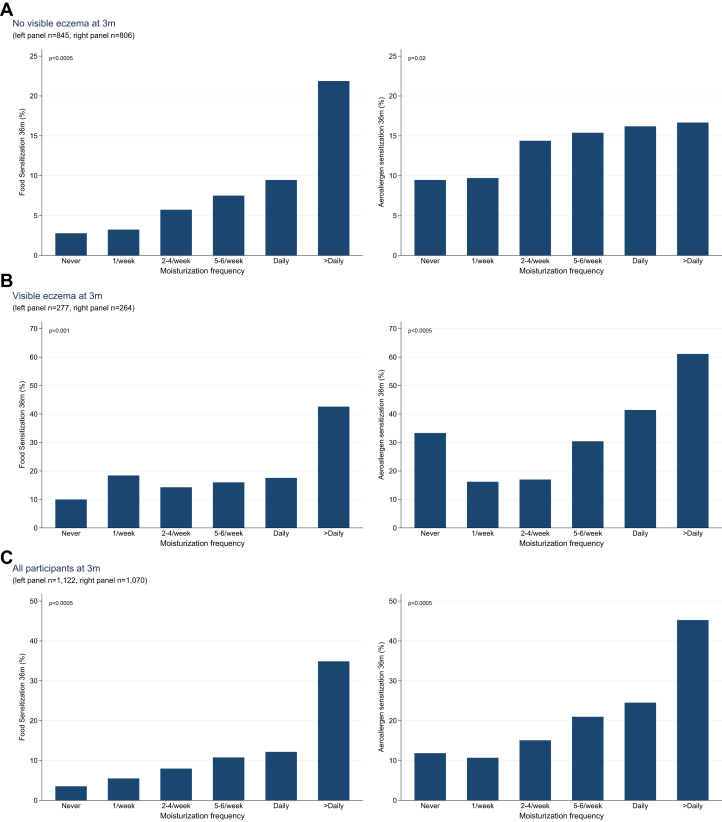
Results: A statistically significant dose-response relationship was observed between parent-reported moisturization frequency at 3 months of age and the subsequent development of food allergy. Each additional moisturization per week was associated with an adjusted odds ratio of 1.20 (95% CI, 1.13-1.27; P < .0005) for developing food allergy. For infants with no visible eczema at the enrollment visit, the corresponding adjusted odds ratio was 1.18 (95% CI, 1.07-1.30; P = .001) and for those with eczema at the enrollment visit, 1.20 (95% CI, 1.11-1.31; P < .0005). Moisturizer frequency showed similar dose-response relationships with the development of both food and aeroallergen sensitization at 36 months.
Conclusions: These findings support the notion that regular application of moisturizers to the skin of young infants may promote the development of food allergy through transcutaneous sensitization.
Keywords: Moisturization; TEWL; allergy prevention; children; eczema; filaggrin; food allergy; skin barrier.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Chemicals in moisturizers may promote type 2 inflammation and food allergy.J Allergy Clin Immunol. 2021 Aug;148(2):652-653. doi: 10.1016/j.jaci.2021.05.010. Epub 2021 Jun 16. J Allergy Clin Immunol. 2021. PMID: 34144818 No abstract available.
-
Reply.J Allergy Clin Immunol. 2021 Aug;148(2):654. doi: 10.1016/j.jaci.2021.04.038. Epub 2021 Jun 16. J Allergy Clin Immunol. 2021. PMID: 34144819 No abstract available.
-
Olive oil is for eating and not skin moisturization.J Allergy Clin Immunol. 2021 Aug;148(2):652. doi: 10.1016/j.jaci.2021.04.037. Epub 2021 Jun 16. J Allergy Clin Immunol. 2021. PMID: 34144820 No abstract available.
-
Potentially harmful substances in moisturizers.J Allergy Clin Immunol. 2021 Aug;148(2):653-654. doi: 10.1016/j.jaci.2021.05.011. Epub 2021 Jun 16. J Allergy Clin Immunol. 2021. PMID: 34144821 No abstract available.
References
-
- Strid J., Hourihane J., Kimber I., Callard R., Strobel S. Epicutaneous exposure to peanut protein prevents oral tolerance and enhances allergic sensitization. Clin Exp Allergy. 2005;35:757–766. - PubMed
-
- Lack G. Epidemiologic risks for food allergy. J Allergy Clin Immunol. 2008;121:1331–1336. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
