

Utility of late pulmonary artery banding in single-ventricle physiology: A mid-term follow-up
- PMID: 33679058
- PMCID: PMC7918013
- DOI: 10.4103/apc.APC_128_20
Utility of late pulmonary artery banding in single-ventricle physiology: A mid-term follow-up
Abstract
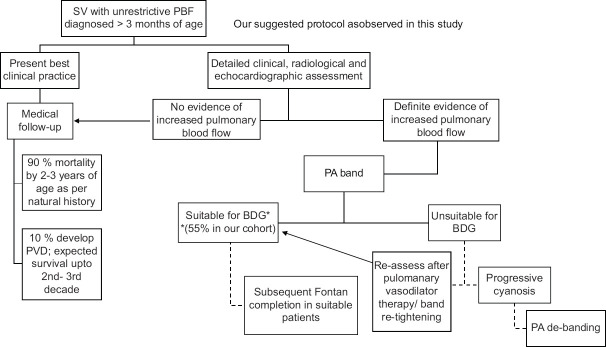
Background: The standard first stage palliation for univentricular heart with unrestricted pulmonary blood flow (PBF) is surgical pulmonary artery (PA) banding for which the ideal age is within the first 8 weeks of life. This study aimed to look for the utility of PA band done beyond 3 months of age for patients presenting beyond the stipulated period.
Materials and methods: This is a retrospective analysis of the outcome of twenty patients with single ventricle (SV) physiology with unrestricted PBF who presented late and were selected on the basis of clinical, radiological, and echocardiographic parameters for PA banding.
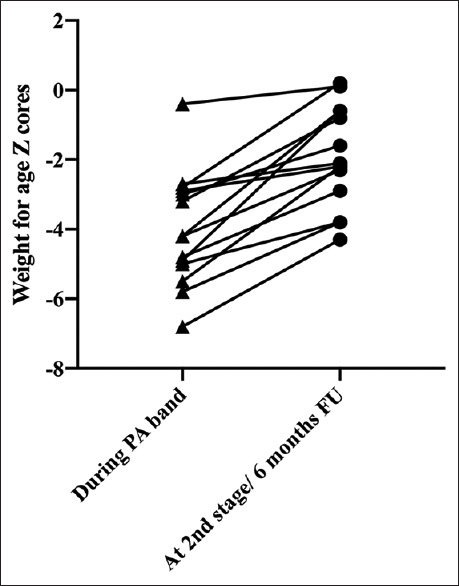
Results: The median age of the patients was 5.5 months (3.5-96 months), and the median body weight was 4.7 kg (3.2-22.0 kg). The patients were divided into three groups as follows: ten patients between 3 and 6 months of age (Group A), seven patients between 6 months to 1 year of age (Group B), and three patients > 1 year of age with additional features of pulmonary venous hypertension (Group C). The mean reduction of PA pressures following PA band was 60.9%, 48.8%, and 58.3% and the mean fall in oxygen saturation was 10.4%, 8.0%, and 6.6% in the three groups, respectively. The postoperative mortality rate was 10%. The mean follow up duration was 13.5 months (7-23 months). There was a statistically significant improvement in weight for age Z scores following PA band (P = 0.0001). On follow up cardiac catheterization, the mean PA pressures were 16.6 (±3.6), 22.7 (±5.7), and 33.3 (±12.4) mmHg, respectively, in the three groups, and the mean pulmonary vascular resistance index was 1.86 (±0.5), 2.45 (±0.7), and 3.5 (±1.6) WU.m2, respectively. Subsequently, seven patients in Group A, three patients in Group B, and one patient from Group C underwent successful bidirectional Glenn (BDG) surgery.
Conclusions: Late PA band in selected patients with SV physiology can have definite benefit in terms of correction of heart failure symptoms and subsequent conversion to BDG and can potentially change the natural history of disease both in terms of survival and quality of life.
Keywords: Late pulmonary artery band; pulmonary vascular disease; single ventricle; unrestrictive pulmonary blood flow.
Copyright: © 2020 Annals of Pediatric Cardiology.
Conflict of interest statement
There are no conflicts of interest.
Figures


References
-
- Rodefeld MD, Ruzmetov M, Schamberger MS, Girod DA, Turrentine MW, Brown JW. Staged surgical repair of functional single ventricle in infants with unobstructed pulmonary blood flow. Eur J Cardiothorac Surg. 2005;27:949–55. - PubMed
-
- Lee MG, Brizard CP, Galati JC, Iyengar AJ, Rakhra SS, Konstantinov IE, et al. Outcomes of patients born with single-ventricle physiology and aortic arch obstruction: The 26-year Melbourne experience. J Thorac Cardiovasc Surg. 2014;148:194–201. - PubMed
-
- Freedom RM, Benson LN, Smallhorn JF, Williams WG, Trusler GA, Rowe RD. Subaortic stenosis, the univentricular heart, and banding of the pulmonary artery: An analysis of the courses of 43 patients with univentricular heart palliated by pulmonary artery banding. Circulation. 1986;73:758–64. - PubMed
-
- Franklin RC, Spiegelhalter DJ, Anderson RH, Macartney FJ, Rossi Filho RI, Rigby ML, et al. Double-inlet ventricle presenting in infancy. II. Results of palliative operations. J Thorac Cardiovasc Surg. 1991;101:917–23. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources