

Re-entrant ventricular tachycardia in a postoperative case of tetralogy of Fallot - Ablated successfully under the three-dimensional mapping system
- PMID: 33679074
- PMCID: PMC7918035
- DOI: 10.4103/apc.APC_84_20
Re-entrant ventricular tachycardia in a postoperative case of tetralogy of Fallot - Ablated successfully under the three-dimensional mapping system
Abstract
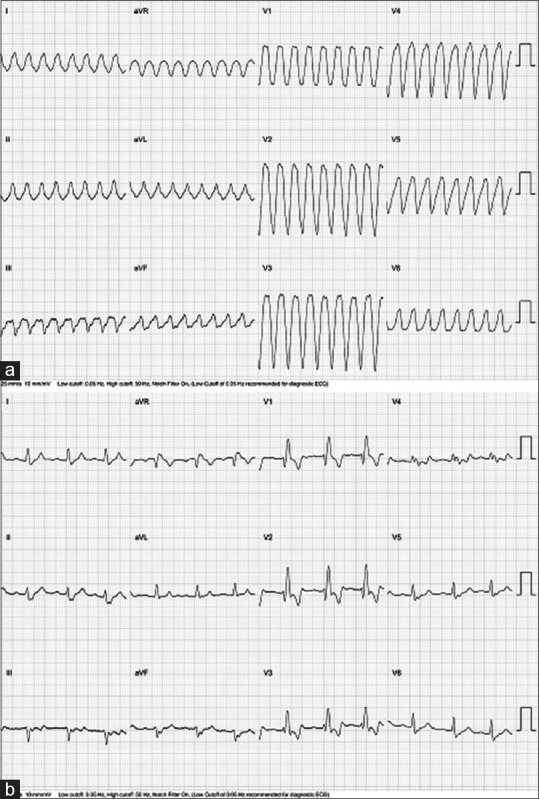
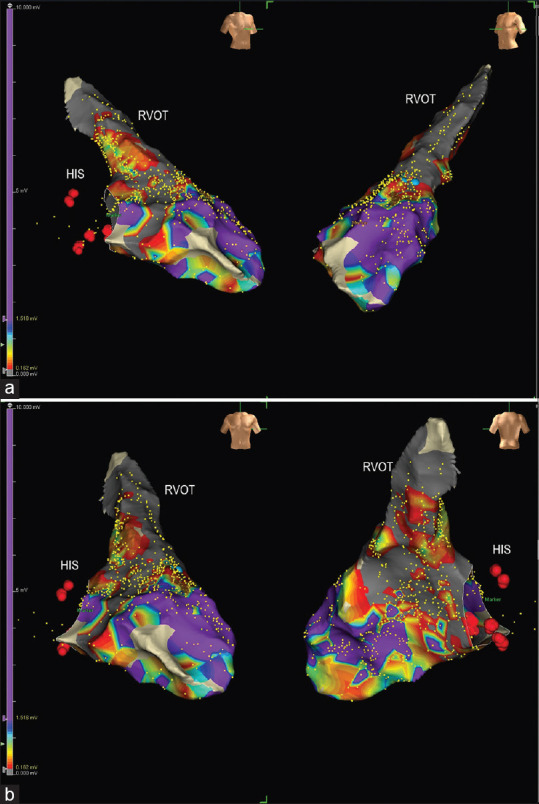
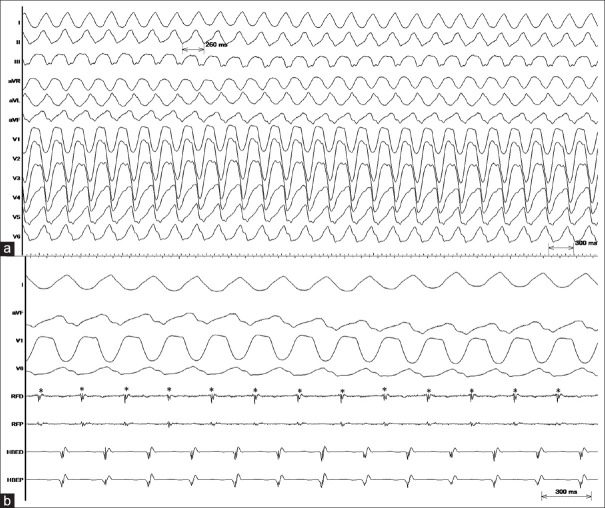
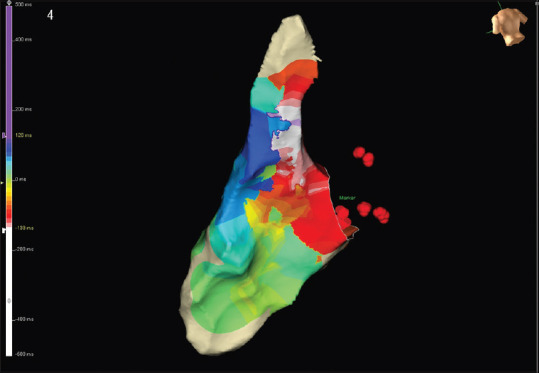
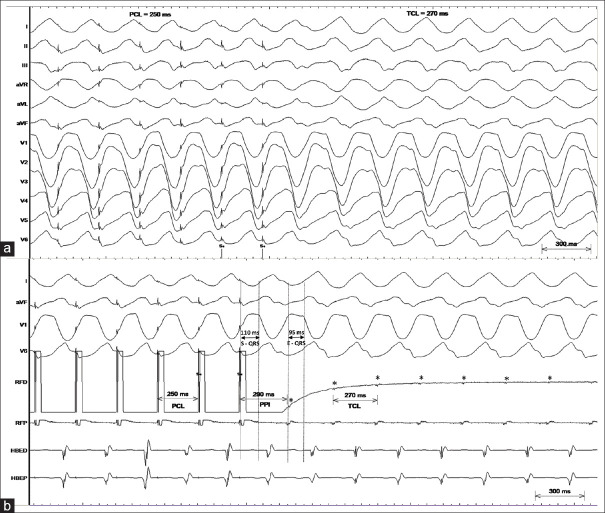
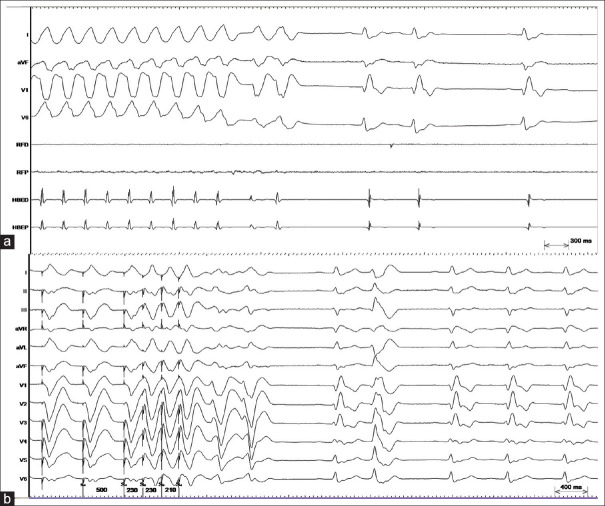
A 47-year-old female underwent cardiac repair for tetralogy of Fallot at the age of 12 years. Subsequently, she was asymptomatic on follow-up. Recently, she presented elsewhere with palpitations and presyncope with documented ventricular tachycardia (VT) having left bundle branch block morphology with inferior QRS axis and late precordial transition. She was reported to have cardioverted and referred to our center for electrophysiology study (EP). She underwent EP study which induced clinical VT which was hemodynamically stable and the mechanism of VT was confirmed as re-entry. With the help of three-dimensional mapping system, VT circuit was identified in the posterior right ventricular outflow tract region between the pulmonary valve and upper end of ventricular septal defect patch. Delivery of radiofrequency energy during VT terminated the tachycardia with no further inducible VT despite aggressive pacing protocols.
Keywords: Catheter ablation; tetralogy of Fallot; ventricular tachycardia.
Copyright: © 2020 Annals of Pediatric Cardiology.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L. Congenital heart disease in the general population: Changing prevalence and age distribution. Circulation. 2007;115:163–72. - PubMed
-
- Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M. Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation. 2014;130:749–56. - PubMed
-
- Diller GP, Kempny A, Liodakis E, Alonso-Gonzalez R, Inuzuka R, Uebing A, et al. Left ventricular longitudinal function predicts life-threatening ventricular arrhythmia and death in adults with repaired tetralogy of fallot. Circulation. 2012;125:2440–6. - PubMed
-
- Kapel GF, Reichlin T, Wijnmaalen AP, Piers SR, Holman ER, Tedrow UB, et al. Re-entry using anatomically determined isthmuses: A curable ventricular tachycardia in repaired congenital heart disease. Circ Arrhythm Electrophysiol. 2015;8:102–9. - PubMed
-
- Zeppenfeld K, Schalij MJ, Bartelings MM, Tedrow UB, Koplan BA, Soejima K, et al. Catheter ablation of ventricular tachycardia after repair of congenital heart disease: Electroanatomic identification of the critical right ventricular isthmus. Circulation. 2007;116:2241–52. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources