

Pharmacological Therapies and Their Clinical Targets in Irritable Bowel Syndrome With Diarrhea
- PMID: 33679391
- PMCID: PMC7935509
- DOI: 10.3389/fphar.2020.629026
Pharmacological Therapies and Their Clinical Targets in Irritable Bowel Syndrome With Diarrhea
Abstract
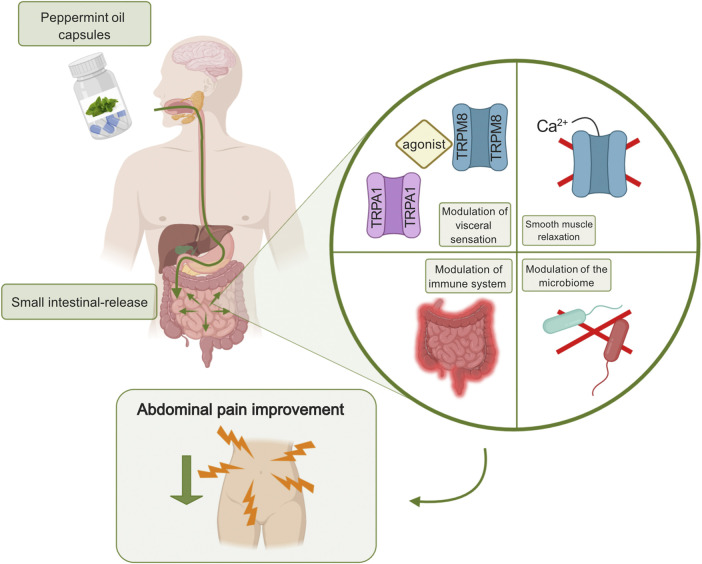
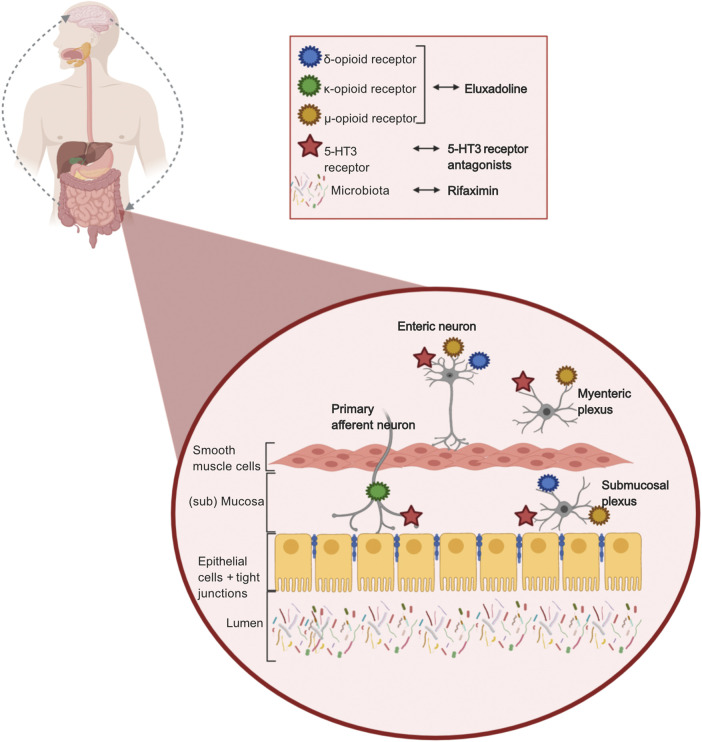
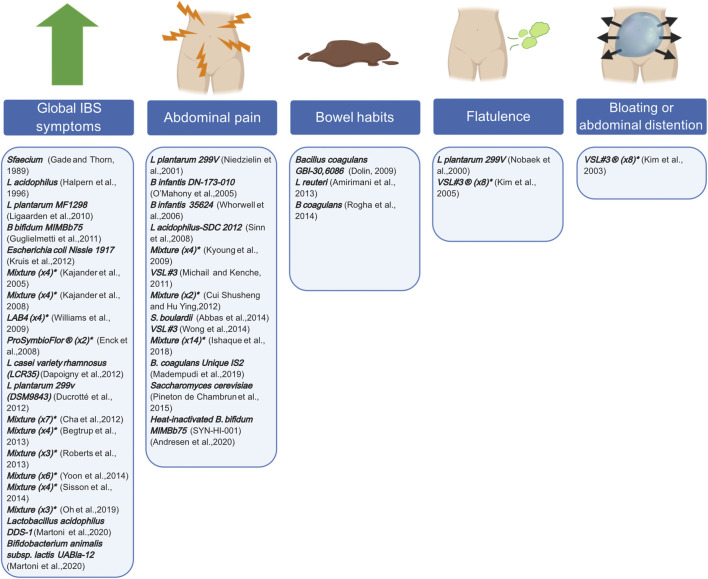
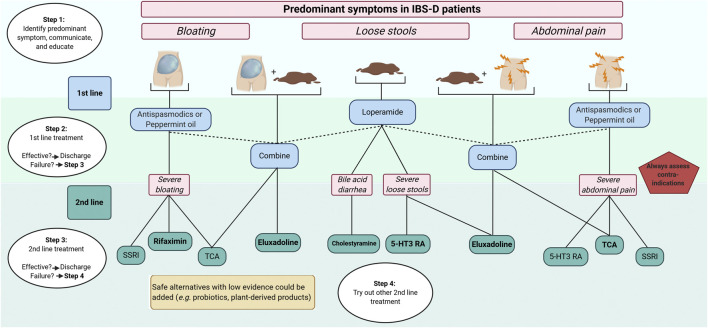
Irritable bowel syndrome (IBS) is one of the most common disorders of the gut-brain axis, which affects approximately 4% of the global population. The Rome IV criteria define IBS as chronic or recurrent abdominal pain associated with altered bowel habits. Patients can be categorized in four subtypes: IBS with predominant constipation (IBS-C), predominant diarrhea (IBS-D), mixed bowel habits (IBS-M), and unclassified (IBS-U). IBS is associated with a lower quality of life, reduced work productivity, and high healthcare costs. When comparing subtypes, patients with IBS-D report lower disease related quality of life. Due to the scope of this review, we have solely focused on patients with IBS-D. Choosing the right pharmacological treatment in these patients remains challenging due to the heterogeneous patient population, patients' expectation of the treatment outcome, unavailability of efficacious drugs, and the multifactorial and incompletely understood underlying pathophysiology. Currently, pharmacological treatment options target individual symptoms, such as abdominal pain, altered bowel habits, and bloating. In this review, we aimed to summarize the current and recent pharmacological treatment options in IBS-D, targeting the predominant gastrointestinal symptoms. Additionally, we proposed a pharmacological treatment algorithm which healthcare professionals could use when treating individual patients with IBS-D.
Keywords: abdominal pain; bloating; clinical management algorithms; diarrhea—therapy; irritable bowel syndrome (IBS); irritable bowel syndrome with diarrhea; loose stools; pharmacology.
Copyright © 2021 Colomier, Algera and Melchior.
Conflict of interest statement
CM has served as Consultant/Advisory Board member for Kyowa Kirin, Norgine, Biocodex, Mayoly spindler, Tillots and Ipsen. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Alammar N., Wang L., Saberi B., Nanavati J., Holtmann G., Shinohara R. T., et al. (2019). The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data 11 medical and health sciences 1103 clinical sciences. BMC Compl. Alternative Med. 19, 21. 10.1186/s12906-018-2409-0 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources