

Neuroprotective Treatment of Postanoxic Encephalopathy: A Review of Clinical Evidence
- PMID: 33679581
- PMCID: PMC7930064
- DOI: 10.3389/fneur.2021.614698
Neuroprotective Treatment of Postanoxic Encephalopathy: A Review of Clinical Evidence
Abstract
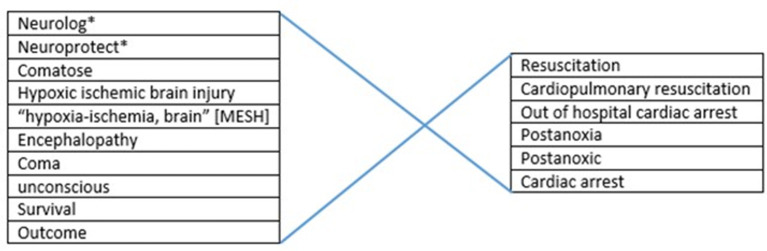
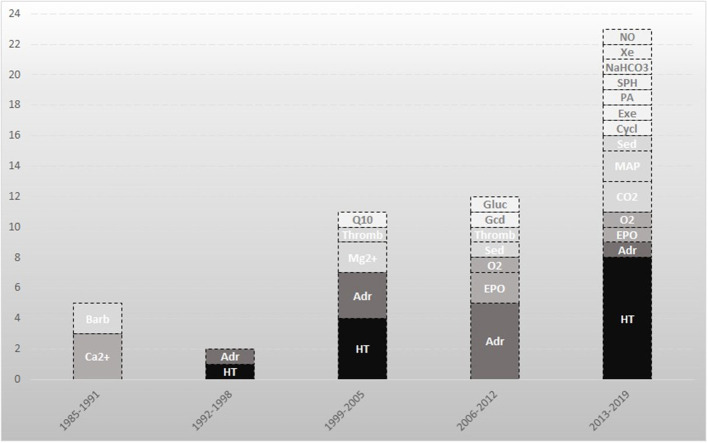
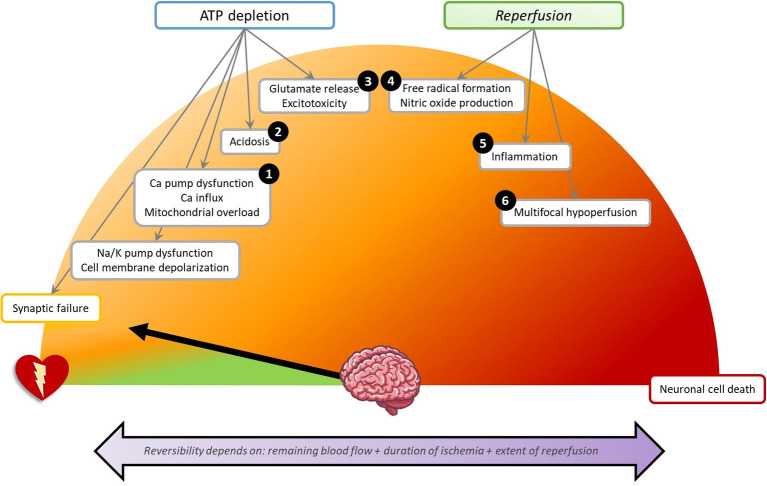
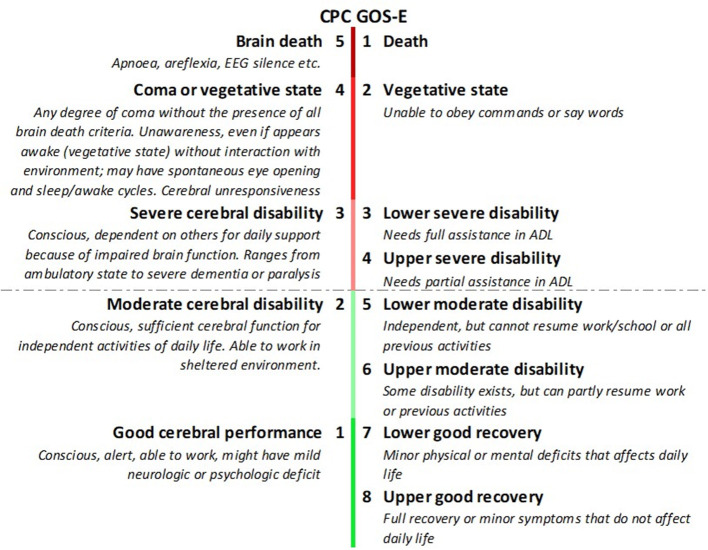
Postanoxic encephalopathy is the key determinant of death or disability after successful cardiopulmonary resuscitation. Animal studies have provided proof-of-principle evidence of efficacy of divergent classes of neuroprotective treatments to promote brain recovery. However, apart from targeted temperature management (TTM), neuroprotective treatments are not included in current care of patients with postanoxic encephalopathy after cardiac arrest. We aimed to review the clinical evidence of efficacy of neuroprotective strategies to improve recovery of comatose patients after cardiac arrest and to propose future directions. We performed a systematic search of the literature to identify prospective, comparative clinical trials on interventions to improve neurological outcome of comatose patients after cardiac arrest. We included 53 studies on 21 interventions. None showed unequivocal benefit. TTM at 33 or 36°C and adrenaline (epinephrine) are studied most, followed by xenon, erythropoietin, and calcium antagonists. Lack of efficacy is associated with heterogeneity of patient groups and limited specificity of outcome measures. Ongoing and future trials will benefit from systematic collection of measures of baseline encephalopathy and sufficiently powered predefined subgroup analyses. Outcome measurement should include comprehensive neuropsychological follow-up, to show treatment effects that are not detectable by gross measures of functional recovery. To enhance translation from animal models to patients, studies under experimental conditions should adhere to strict methodological and publication guidelines.
Keywords: cerebral ischaemia; hypoxic ischaemic brain injury; post-cardiac arrest syndrome; postanoxic coma; resuscitation.
Copyright © 2021 Nutma, le Feber and Hofmeijer.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Effects of targeted temperature management at 33 °C vs. 36 °C on comatose patients after cardiac arrest stratified by the severity of encephalopathy.Resuscitation. 2022 Apr;173:147-153. doi: 10.1016/j.resuscitation.2022.01.026. Epub 2022 Feb 2. Resuscitation. 2022. PMID: 35122892
-
Early neuroprotection after cardiac arrest.Curr Opin Crit Care. 2014 Jun;20(3):250-8. doi: 10.1097/MCC.0000000000000086. Curr Opin Crit Care. 2014. PMID: 24717694 Review.
-
Impact of time to return of spontaneous circulation on neuroprotective effect of targeted temperature management at 33 or 36 degrees in comatose survivors of out-of hospital cardiac arrest.Resuscitation. 2015 Nov;96:310-6. doi: 10.1016/j.resuscitation.2015.06.021. Epub 2015 Jul 7. Resuscitation. 2015. PMID: 26159609 Clinical Trial.
-
Predictive value of EEG in postanoxic encephalopathy: A quantitative model-based approach.Resuscitation. 2017 Oct;119:27-32. doi: 10.1016/j.resuscitation.2017.07.020. Epub 2017 Jul 24. Resuscitation. 2017. PMID: 28750884
-
A practical approach to the use of targeted temperature management after cardiac arrest.Minerva Anestesiol. 2020 Oct;86(10):1103-1110. doi: 10.23736/S0375-9393.20.14399-2. Epub 2020 May 28. Minerva Anestesiol. 2020. PMID: 32463209 Review.
Cited by
-
MLC901 in hypoxic-ischemic brain injury patients: A double-blind, randomized placebo-controlled pilot study.Medicine (Baltimore). 2023 Jun 9;102(23):e33914. doi: 10.1097/MD.0000000000033914. Medicine (Baltimore). 2023. PMID: 37335674 Free PMC article. Clinical Trial.
-
Etiology and Functional Outcomes following Hypoxic Ischemic Encephalopathy in Adults: A 10-Year Retrospective Cohort Study.Arch Rehabil Res Clin Transl. 2024 Dec 19;7(1):100418. doi: 10.1016/j.arrct.2024.100418. eCollection 2025 Mar. Arch Rehabil Res Clin Transl. 2024. PMID: 40463768 Free PMC article.
-
Recovery and Survival of Patients After Out-of-Hospital Cardiac Arrest: A Literature Review Showcasing the Big Picture of Intensive Care Unit-Related Factors.Cureus. 2024 Feb 24;16(2):e54827. doi: 10.7759/cureus.54827. eCollection 2024 Feb. Cureus. 2024. PMID: 38529434 Free PMC article. Review.
-
Evolution of brain injury and neurological dysfunction after cardiac arrest in the rat - A multimodal and comprehensive model.J Cereb Blood Flow Metab. 2024 Nov;44(11):1316-1329. doi: 10.1177/0271678X241255599. Epub 2024 May 21. J Cereb Blood Flow Metab. 2024. PMID: 38770566 Free PMC article.
-
Wolf Creek XVII Part 8: Neuroprotection.Resusc Plus. 2024 Feb 1;17:100556. doi: 10.1016/j.resplu.2024.100556. eCollection 2024 Mar. Resusc Plus. 2024. PMID: 38328750 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources