

Immune Deregulation in Sepsis and Septic Shock: Reversing Immune Paralysis by Targeting PD-1/PD-L1 Pathway
- PMID: 33679715
- PMCID: PMC7925640
- DOI: 10.3389/fimmu.2020.624279
Immune Deregulation in Sepsis and Septic Shock: Reversing Immune Paralysis by Targeting PD-1/PD-L1 Pathway
Abstract
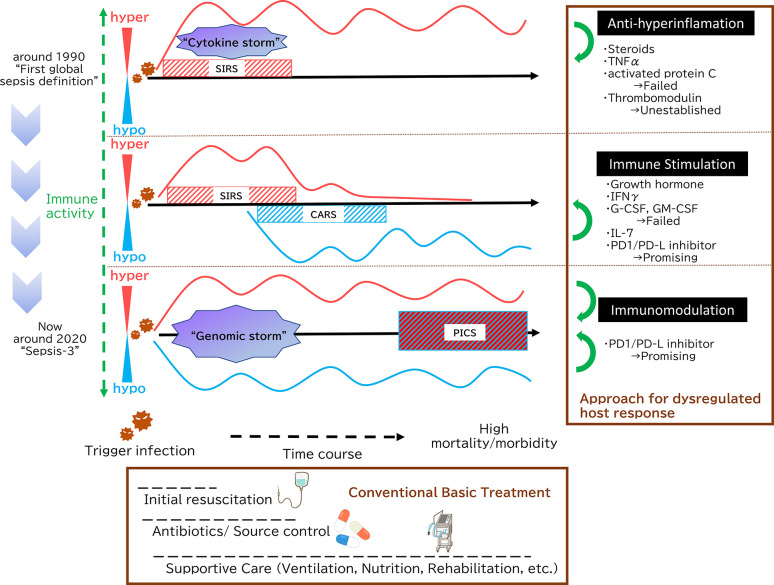
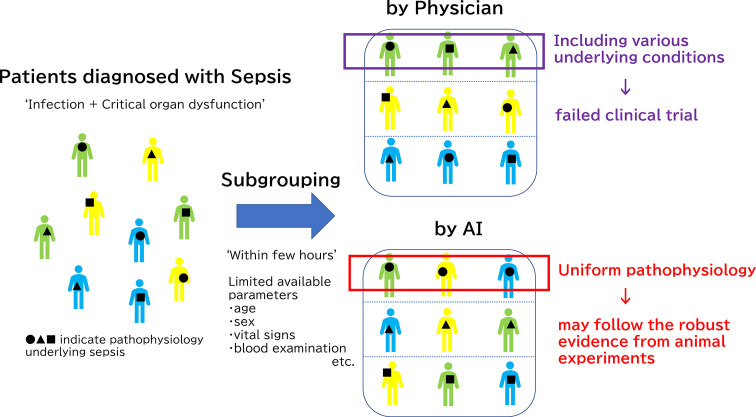
Sepsis remains a major problem for human health worldwide, thereby manifesting high rates of morbidity and mortality. Sepsis, once understood as a monophasic sustained hyperinflammation, is currently recognized as a dysregulated host response to infection, with both hyperinflammation and immunoparalysis occurring simultaneously from the earliest stages of sepsis, involving multiple organ dysfunctions. Despite the recent progress in the understanding of the pathophysiology underlying sepsis, no specific treatment to restore immune dysregulation in sepsis has been validated in clinical trials. In recent years, treatment for immune checkpoints such as the programmed cell death protein 1/programmed death ligand (PD-1/PD-L) pathway in tumor-infiltrating T-lymphocytes has been successful in the field of cancer immune therapy. As immune-paralysis in sepsis involves exhausted T-lymphocytes, future clinical applications of checkpoint inhibitors for sepsis are expected. In addition, the functions of PD-1/PD-L on innate lymphoid cells and the role of exosomal forms of PD-L1 warrant further research. Looking back on the history of repeatedly failed clinical trials of immune modulatory therapies for sepsis, sepsis must be recognized as a difficult disease entity for performing clinical trials. A major obstacle that could prevent effective clinical trials of drug candidates is the disease complexity and heterogeneities; clinically diagnosed sepsis could contain multiple sepsis subgroups that suffer different levels of hyper-inflammation and immune-suppression in distinct organs. Thus, the selection of appropriate more homogenous sepsis subgroup is the key for testing the clinical efficacy of experimental therapies targeting specific pathways in either hyperinflammation and/or immunoparalysis. An emerging technology such as artificial intelligence (AI) may help to identify an immune paralysis subgroup who would best be treated by PD-1/PD-L1 pathway inhibitors.
Keywords: PD-1; PD-L; artificial intelligence; immune checkpoints inhibitors; immunomodulation; immunoparalysis; machine learning; sepsis - diagnostics.
Copyright © 2021 Nakamori, Park and Shimaoka.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Frontline Science: Defects in immune function in patients with sepsis are associated with PD-1 or PD-L1 expression and can be restored by antibodies targeting PD-1 or PD-L1.J Leukoc Biol. 2016 Dec;100(6):1239-1254. doi: 10.1189/jlb.4HI0616-255R. Epub 2016 Sep 26. J Leukoc Biol. 2016. PMID: 27671246 Free PMC article.
-
PD-1/PD-L1 Blockade Therapy in Advanced Non-Small-Cell Lung Cancer: Current Status and Future Directions.Oncologist. 2019 Feb;24(Suppl 1):S31-S41. doi: 10.1634/theoncologist.2019-IO-S1-s05. Oncologist. 2019. PMID: 30819829 Free PMC article. Review.
-
The Role of Programmed Cell Death 1/Programmed Death Ligand 1 (PD-1/PD-L1) Axis in Sepsis-Induced Apoptosis.Medicina (Kaunas). 2024 Jul 19;60(7):1174. doi: 10.3390/medicina60071174. Medicina (Kaunas). 2024. PMID: 39064603 Free PMC article.
-
The implication of targeting PD-1:PD-L1 pathway in treating sepsis through immunostimulatory and anti-inflammatory pathways.Front Immunol. 2023 Dec 13;14:1323797. doi: 10.3389/fimmu.2023.1323797. eCollection 2023. Front Immunol. 2023. PMID: 38193090 Free PMC article. Review.
-
PD-1 signaling pathway in sepsis: Does it have a future?Clin Immunol. 2021 Aug;229:108742. doi: 10.1016/j.clim.2021.108742. Epub 2021 Apr 24. Clin Immunol. 2021. PMID: 33905818 Review.
Cited by
-
PD-1/PD-L1 blockade abrogates a dysfunctional innate-adaptive immune axis in critical β-coronavirus disease.Sci Adv. 2022 Sep 23;8(38):eabn6545. doi: 10.1126/sciadv.abn6545. Epub 2022 Sep 21. Sci Adv. 2022. PMID: 36129987 Free PMC article.
-
Acute respiratory distress syndrome heterogeneity and the septic ARDS subgroup.Front Immunol. 2023 Nov 14;14:1277161. doi: 10.3389/fimmu.2023.1277161. eCollection 2023. Front Immunol. 2023. PMID: 38035100 Free PMC article. Review.
-
Composition, functions, and applications of exosomal membrane proteins.Front Immunol. 2024 Aug 1;15:1408415. doi: 10.3389/fimmu.2024.1408415. eCollection 2024. Front Immunol. 2024. PMID: 39148736 Free PMC article. Review.
-
Mechanisms of Sepsis-Induced Acute Lung Injury and Advancements of Natural Small Molecules in Its Treatment.Pharmaceuticals (Basel). 2024 Apr 8;17(4):472. doi: 10.3390/ph17040472. Pharmaceuticals (Basel). 2024. PMID: 38675431 Free PMC article. Review.
-
Severity of Sepsis Determines the Degree of Impairment Observed in Circulatory and Tissue-Resident Memory CD8 T Cell Populations.J Immunol. 2021 Oct 1;207(7):1871-1881. doi: 10.4049/jimmunol.2001142. Epub 2021 Sep 3. J Immunol. 2021. PMID: 34479943 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials