

Comparison of whole-body vibration training and quadriceps strength training on physical function and neuromuscular function of individuals with knee osteoarthritis: A randomised clinical trial
- PMID: 33680003
- PMCID: PMC7895843
- DOI: 10.1016/j.jesf.2021.01.003
Comparison of whole-body vibration training and quadriceps strength training on physical function and neuromuscular function of individuals with knee osteoarthritis: A randomised clinical trial
Abstract
Background: Knee osteoarthritis (KOA) is one of the leading causes of global disability, which causes knee pain, stiffness and swelling. Impaired neuromuscular function may cause joint instability, alignment changes and knee stress, which leads to the progression of KOA. Whole-body vibration (WBV) training is considered to improve pain and functional mobility effectively. However, few studies have investigated the therapeutic effect of WBV on neuromuscular function in KOA.
Material and methods: A single-blinded, randomised, controlled trial was performed on 81 participants diagnosed with KOA. The participants were randomised into three groups: (1) WBV group, in which participants performed strength training (ST) with vibration exposure for 8 weeks; (2) ST group, in which participants performed ST without vibration for 8 weeks; and (3) health education (HE) group, in which participants received a HE for 8 weeks. The visual analogue scale for knee pain, isokinetic muscle strength test, proprioception test, Timed Up and Go test (TUG) and 6-min Walk Distance test (6MWD) were performed before and after the interventions.
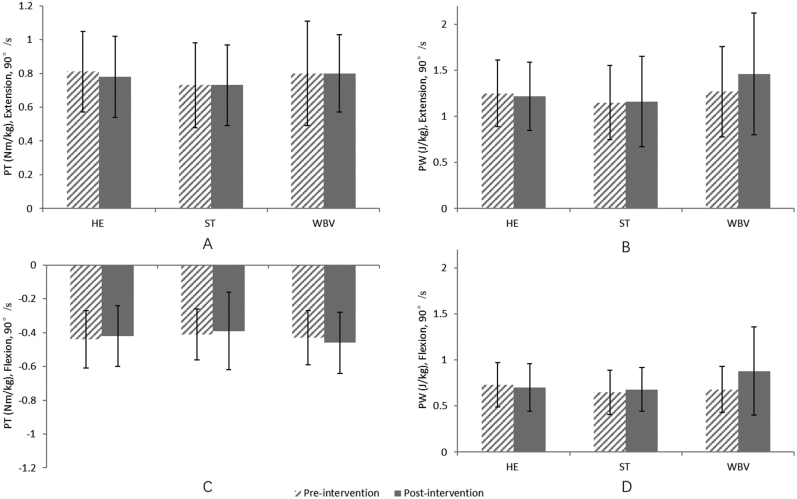
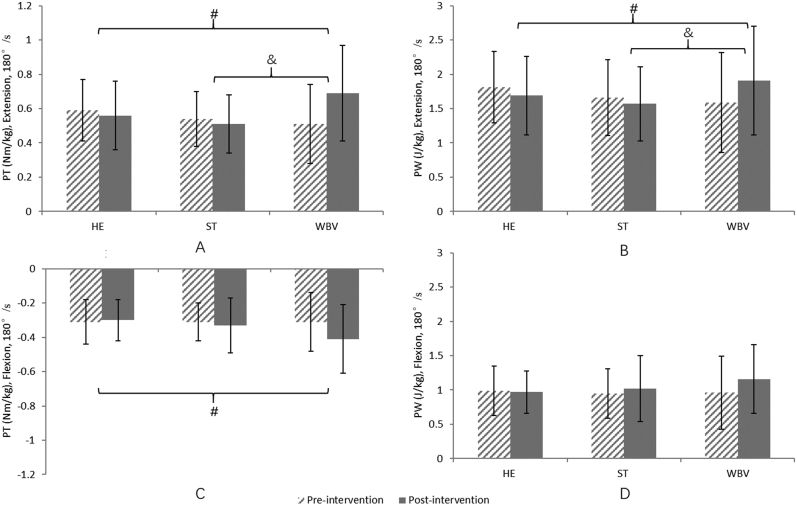
Results: No significant difference was found on pain, proprioception, TUG and 6MWD. A significant interaction effect was found in isokinetic muscle strength between groups. Further analysis showed that compared with the HE group, the WBV group exhibited significantly greater improvement in isokinetic muscle strength (peak torque [PT] of extensors, p < 0.01, 95% CI = 0.11-0.33 Nm/kg; PT of flexors, p = 0.01, 95% CI = 0.02-0.19 Nm/kg; peak work [PW] of extensors, p < 0.01, 95% CI = 0.12-0.75 W/kg). In addition, compared with the ST group, the muscle strength of the WBV group (PT of extensors, p < 0.01, 95% CI = 0.10-0.32 Nm/kg; PW of extensors, p < 0.01, 95% CI = 0.09-0.71 W/kg) improved significantly.
Conclusion: Our findings suggested that adding WBV training to ST might benefit muscle strength around the knee joint in patients with KOA.
Keywords: Knee; Muscle strength; Physical therapy; Proprioception.
© 2021 The Society of Chinese Scholars on Exercise Physiology and Fitness. Published by Elsevier (Singapore) Pte Ltd.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures

References
-
- Ferreira R.M., Duarte J.A., Goncalves R.S. Non-pharmacological and non-surgical interventions to manage patients with knee osteoarthritis: an umbrella review. Acta Reumatol Port. 2018;43:182–200. - PubMed
-
- Cross M., Smith E., Hoy D. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–1330. - PubMed
-
- Bijlsma J.W., Berenbaum F., Lafeber F.P. Osteoarthritis: an update with relevance for clinical practice. Lancet. 2011;377:2115–2126. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
