

Automated Procedure Logs for Cardiology Fellows: A New Training Paradigm in the Era of Electronic Health Records
- PMID: 33680308
- PMCID: PMC7901634
- DOI: 10.4300/JGME-D-20-00642.1
Automated Procedure Logs for Cardiology Fellows: A New Training Paradigm in the Era of Electronic Health Records
Abstract
Background: Procedural experience for residents and fellows is critical for achieving competence, and documentation of procedures performed is required. Procedure logs serve as the record of this experience, but are commonly generated manually, require substantial administrative effort, and cannot be corroborated for accuracy.
Objective: We developed and implemented a structured clinical-educational report template (CERT), which automatically generates procedure logs directly from the clinical record.
Methods: Our CERT aimed to replace the post-procedure note template for our cardiac catheterization laboratory and was incorporated into the electronic health record system. Numbers of documented procedures in automated CERT-derived procedure logs over a 1-year post-intervention period (2018-2019) were compared to manual logs and corrected for clinical volume changes. The CERT's impact on fellowship experience was also assessed.
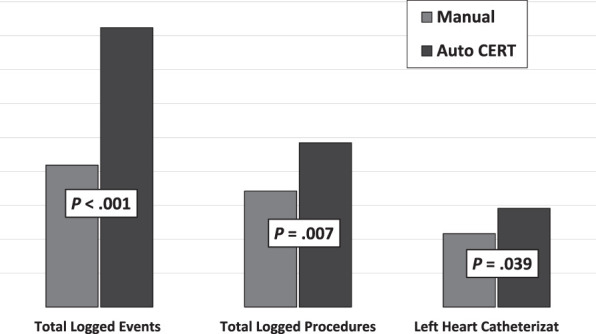
Results: Automated CERT procedure logs increased weekly procedural documentation over manual procedure logs for total procedures (24.2 ± 6.1 vs 17.1 ± 6.8, P = .007), left heart catheterizations (14.5 ± 3.6 vs 10.8 ± 4.2, P = .039), total procedural elements (40.2 ± 11.4 versus 20.9 ± 12.5, P < .001), and captured procedural details not previously documented. The CERT also reduced self-reported administrative time and improved fellowship experience.
Conclusions: A novel CERT allows procedure logs to be automatically derived from the clinical record and increased the number of documented procedures, compared to manual logging. This innovation ensures an accurate record of procedural experience and reduces self-reported non-educational administrative time for cardiology fellows.
Conflict of interest statement
Conflict of interest: The authors declare they have no competing interests.
Figures

Similar articles
-
Diagnostic coronary angiography: initial results of a simulation program.Cardiovasc Revasc Med. 2016 Mar;17(2):102-5. doi: 10.1016/j.carrev.2015.12.010. Epub 2015 Dec 28. Cardiovasc Revasc Med. 2016. PMID: 26811001
-
A novel use of the discrete templated notes within an electronic health record software to monitor resident supervision.J Am Med Inform Assoc. 2017 Apr 1;24(e1):e2-e8. doi: 10.1093/jamia/ocw078. J Am Med Inform Assoc. 2017. PMID: 27274023 Free PMC article.
-
General Surgery Resident Case Logs: Do They Accurately Reflect Resident Experience?J Surg Educ. 2015 Nov-Dec;72(6):e178-83. doi: 10.1016/j.jsurg.2015.04.022. J Surg Educ. 2015. PMID: 26073716
-
Evaluating Coding Accuracy in General Surgery Residents' Accreditation Council for Graduate Medical Education Procedural Case Logs.J Surg Educ. 2016 Nov-Dec;73(6):e59-e63. doi: 10.1016/j.jsurg.2016.07.017. J Surg Educ. 2016. PMID: 27886974 Review.
-
How the COVID-19 Pandemic Has Affected Cardiology Fellow Training.Am J Cardiol. 2021 Jul 15;151:114-117. doi: 10.1016/j.amjcard.2021.03.052. Epub 2021 Apr 15. Am J Cardiol. 2021. PMID: 34052015 Free PMC article. Review.
Cited by
-
To the Editor: Incorporating New Technologies Into Graduate Medical Education Practices.J Grad Med Educ. 2021 Aug;13(4):591. doi: 10.4300/JGME-D-21-00366.1. Epub 2021 Aug 13. J Grad Med Educ. 2021. PMID: 34434525 Free PMC article. No abstract available.
-
Improving ACGME Compliance for Obstetric Anesthesiology Fellows Using an Automated Email Notification System.Appl Clin Inform. 2021 May;12(3):479-483. doi: 10.1055/s-0041-1730323. Epub 2021 May 26. Appl Clin Inform. 2021. PMID: 34041735 Free PMC article.
-
Implementation and Evaluation of Integrating an Electronic Health Record With the ACGME Case Log System.J Grad Med Educ. 2022 Aug;14(4):482-487. doi: 10.4300/JGME-D-22-00021.1. J Grad Med Educ. 2022. PMID: 35991093 Free PMC article.
-
Charting Tomorrow's Healthcare: A Traditional Literature Review for an Artificial Intelligence-Driven Future.Cureus. 2024 Apr 11;16(4):e58032. doi: 10.7759/cureus.58032. eCollection 2024 Apr. Cureus. 2024. PMID: 38738104 Free PMC article. Review.
References
-
- Sanborn TA, Tcheng JE, Anderson HV, Chambers CE, Cheatham SL, DeCaro MV, et al. ACC/AHA/SCAI 2014 health policy statement on structured reporting for the cardiac catheterization laboratory: a report of the American College of Cardiology Clinical Quality Committee. Circulation. 2014;129(24):2578–609. doi: 10.1161/CIR.0000000000000043. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources