

Primary vulvar leiomyosarcoma localized in the Bartholin's gland area: A case report and review
- PMID: 33680460
- PMCID: PMC7890440
- DOI: 10.3892/mco.2021.2231
Primary vulvar leiomyosarcoma localized in the Bartholin's gland area: A case report and review
Abstract
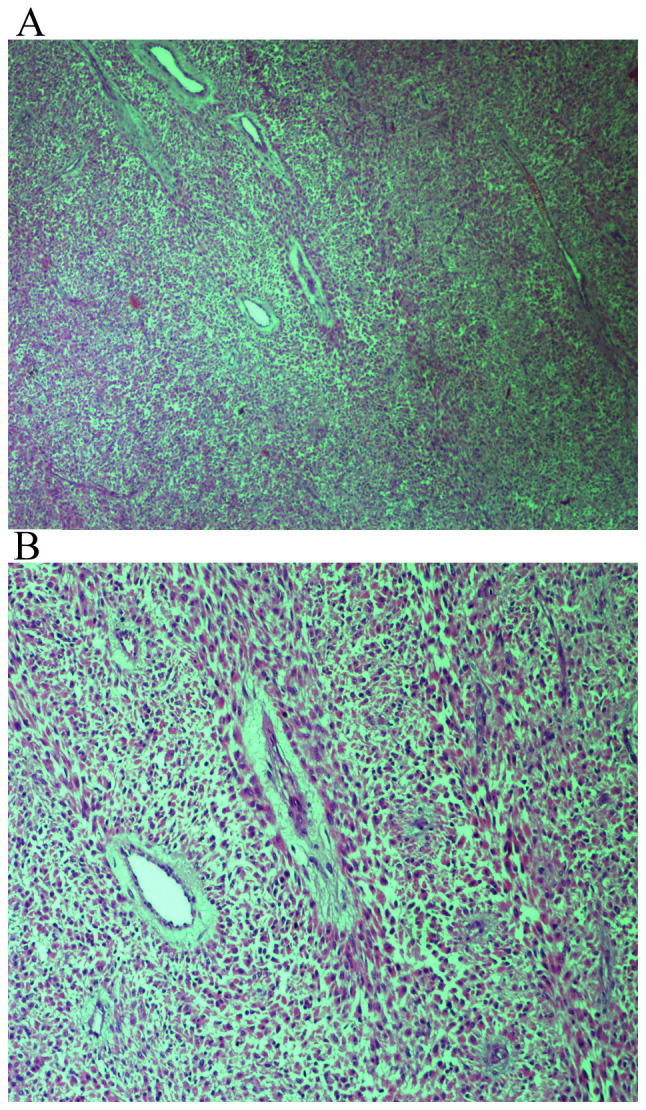
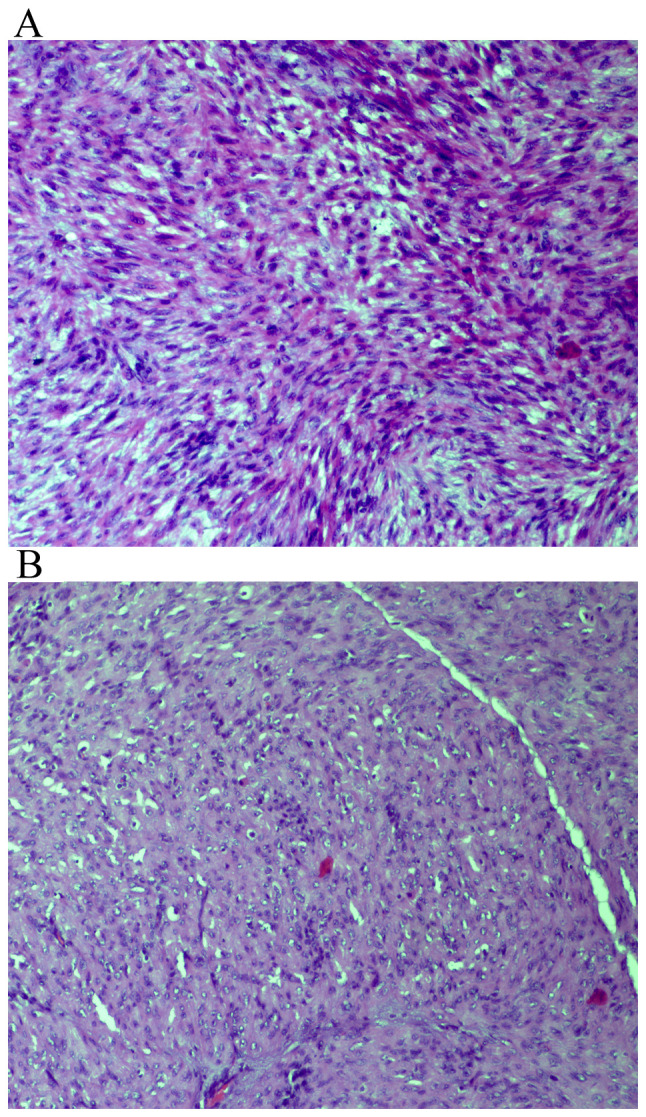
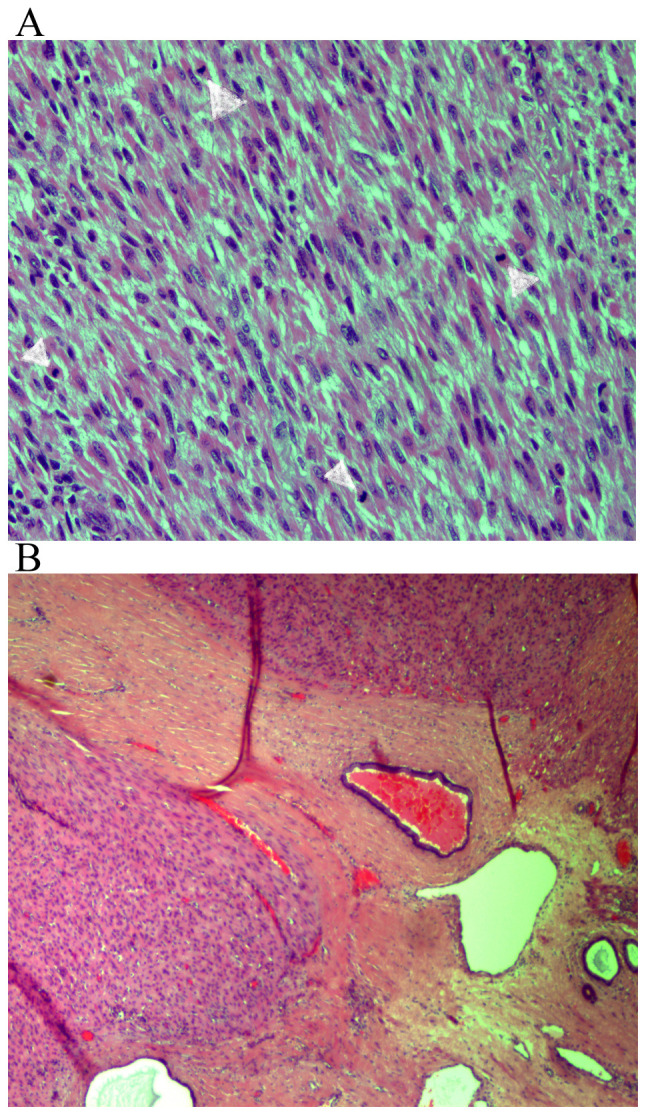
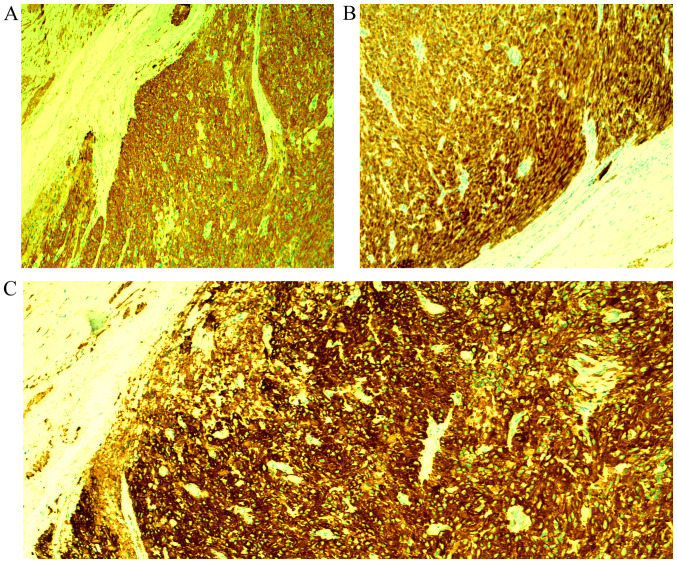
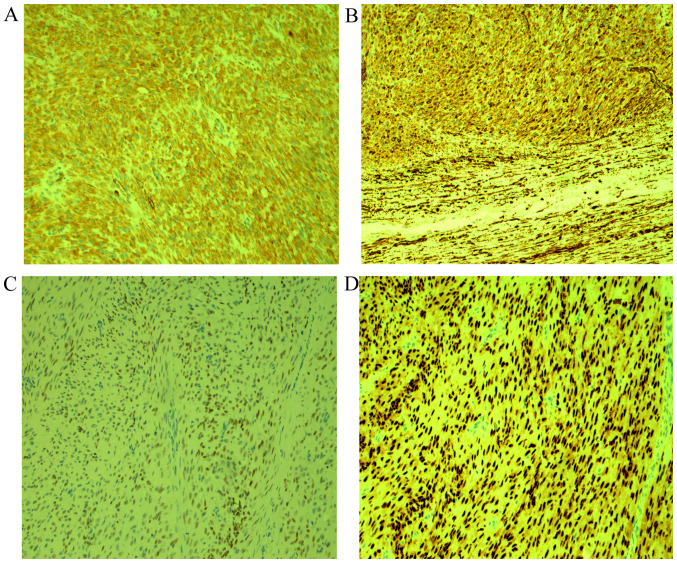
Vulvar sarcomas located in the Bartholin's gland area are extremely uncommon mesenchymal vulvar tumors. These neoplasms can be mistaken as Bartholin' gland benign lesions such as cysts or abscesses, leading to a delay in the diagnosis of underlying malignancy. Currently, only a few cases of these aggressive cancers have been reported in the literature. A 42-year-old female patient without any previous complaint presented to Obstetrics and Gynecology Department of 'G. Chaztikosta' General Hospital due to a vulvar lump in the area of the left Bartholin's gland with a 6-month history of progressive swelling. Pelvic examination showed a solid mass of 6.5-cm in maximum diameter, localized in the left Bartholin's gland. The patient underwent wide local excision and histopathological examination of hematoxylin and eosin-stained sections indicated intersecting fascicles of spindle cells, with moderate to severe atypia. The number of mitoses was up to 8 per 10 high power fields. The neoplasm to its greatest extent was circumscribed and in places had an invasive growth pattern. Tumoral necrosis was not seen. Involved Bartholin' gland by the tumor was identified. The tumor extended focally to the surgical margin. The neoplastic cells showed positive staining for smooth muscle actin, desmin, HHF35, caldesmon, vimentin and estrogen and progesterone receptors. Immunohistochemistry was negative for S100, myoglobulin, keratin 116, CD117, CD34 and CD31. The patient denied further surgery or/and local radiotherapy, although the mass was >5-cm and a focally infiltrative surgical margin was found. During the close follow-up, no local recurrences or metastases were observed 53 months after surgery. In conclusion, wide local tumor excision with free surgical margins is a good option of surgery for vulvar leiomyosarcomas. In recurrences, a new extensive surgical resection of the lesion and radiotherapy are suggested. Ipsilateral lympadenectomy is indicated when there is a pathologic lymph node. Chemotherapy is provided in cases of distal metastases.
Keywords: Bartholin's gland; leiomyosarcoma; soft tissue; vulva; vulvar diseases; vulvar neoplasm; vulvar sarcoma.
Copyright: © Akrivi et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A rare case of leiomyosarcoma localized in the Bartholin's gland area and review of the literature.J Obstet Gynaecol Res. 2016 May;42(5):589-592. doi: 10.1111/jog.12943. Epub 2016 Feb 18. J Obstet Gynaecol Res. 2016. PMID: 26889877
-
Vulvar leiomyosarcoma in Bartholin's gland area: a case report and literature review.Arch Gynecol Obstet. 2009 Feb;279(2):171-4. doi: 10.1007/s00404-008-0652-1. Epub 2008 Apr 24. Arch Gynecol Obstet. 2009. PMID: 18437406 Review.
-
Leiomyosarcoma of the Vulva Mimicking as Chronic Bartholin Cyst: A Case Report.Oman Med J. 2020 Jul 29;35(4):e153. doi: 10.5001/omj.2020.74. eCollection 2020 Jul. Oman Med J. 2020. PMID: 32760601 Free PMC article.
-
Nodular hyperplasia, adenoma, and adenomyoma of Bartholin's gland.Int J Gynecol Pathol. 1998 Oct;17(4):289-94. doi: 10.1097/00004347-199810000-00001. Int J Gynecol Pathol. 1998. PMID: 9785128
-
Adenoid cystic carcinoma of Bartholin's Gland. Case report with review of the literature.Gynecol Obstet Invest. 2005;59(1):54-8. doi: 10.1159/000081468. Epub 2004 Oct 12. Gynecol Obstet Invest. 2005. PMID: 15479983 Review.
Cited by
-
Vulvar Leiomyosarcomas: A Case Series with Clinical Comparison to Uterine Leiomyosarcomas and Review of the Literature.Am J Case Rep. 2023 May 27;24:e939402. doi: 10.12659/AJCR.939402. Am J Case Rep. 2023. PMID: 37243328 Free PMC article. Review.
-
Vulvar Leiomyosarcoma in Pregnancy.Cureus. 2021 Oct 14;13(10):e18772. doi: 10.7759/cureus.18772. eCollection 2021 Oct. Cureus. 2021. PMID: 34796063 Free PMC article.
-
Common and uncommon lesions of the vulva and vagina on magnetic resonance imaging: correlations with pathological findings.BJR Open. 2023 Jun 28;5(1):20230002. doi: 10.1259/bjro.20230002. eCollection 2023. BJR Open. 2023. PMID: 37389007 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources