

Colon phantoms with cancer lesions for endoscopic characterization with optical coherence tomography
- PMID: 33680552
- PMCID: PMC7901311
- DOI: 10.1364/BOE.402081
Colon phantoms with cancer lesions for endoscopic characterization with optical coherence tomography
Abstract
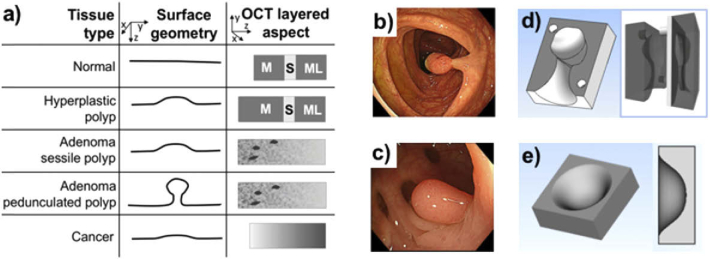
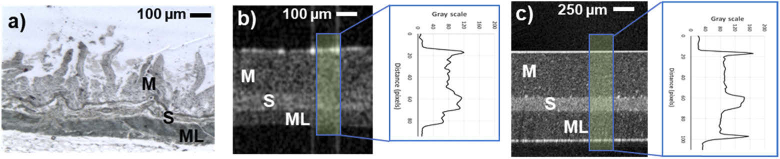
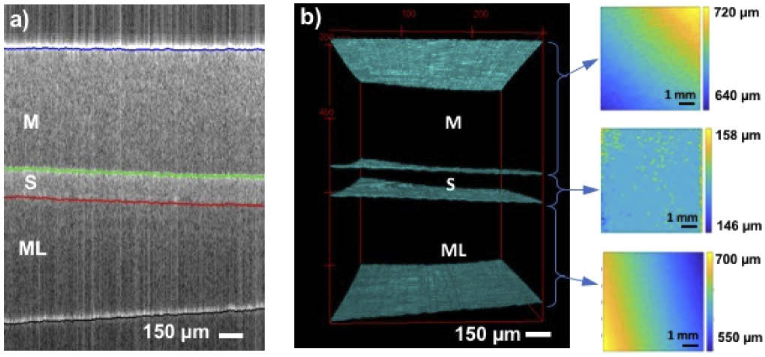
Optical coherence tomography (OCT) is a growing imaging technique for real-time early diagnosis of digestive system diseases. As with other well-established medical imaging modalities, OCT requires validated imaging performance and standardized test methods for performance assessment. A major limitation in the development and testing of new imaging technologies is the lack of models for simultaneous clinical procedure emulation and characterization of healthy and diseased tissues. Currently, the former can be tested in large animal models and the latter can be tested in small animal disease models or excised human biopsy samples. In this study, a 23 cm by 23 cm optical phantom was developed to mimic the thickness and near-infrared optical properties of each anatomical layer of a human colon, as well as the surface topography of colorectal polyps and visual appearance compatible with white light endoscopy.
© 2021 Optical Society of America under the terms of the OSA Open Access Publishing Agreement.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures





References
-
- Gora M. J., Sauk J. S., Carruth R. W., Gallagher K. A., Suter M. J., Nishioka N. S., Kava L. E., Rosenberg M., Bouma B. E., Tearney G. J., “Tethered capsule endomicroscopy enables less invasive imaging of gastrointestinal tract microstructure,” Nat. Med. 19(2), 238–240 (2013). 10.1038/nm.3052 - DOI - PMC - PubMed
-
- Jäckle S., Gladkova N., Feldchtein F., Terentieva A., Brand B., Gelikonov G., Gelikonov V., Sergeev A., Fritscher-Ravens A., Freund J., Seitz U., Soehendra S., Schrödern N., “In vivo endoscopic optical coherence tomography of the human gastrointestinal tract–toward optical biopsy,” Endoscopy 32(10), 743–749 (2000). 10.1055/s-2000-7711 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials