

A Novel Technique for Single-stage Reconstruction of Nipple-Areola Complex following Central Lumpectomy
- PMID: 33680650
- PMCID: PMC7928539
- DOI: 10.1097/GOX.0000000000003397
A Novel Technique for Single-stage Reconstruction of Nipple-Areola Complex following Central Lumpectomy
Abstract
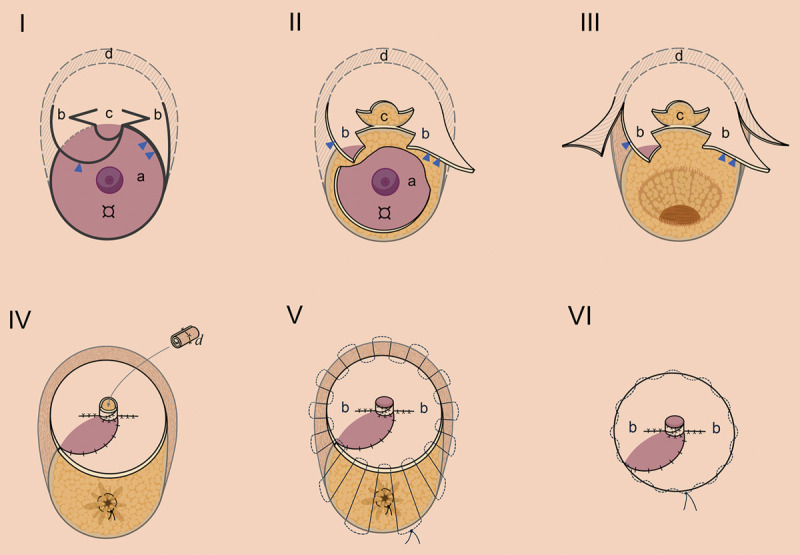
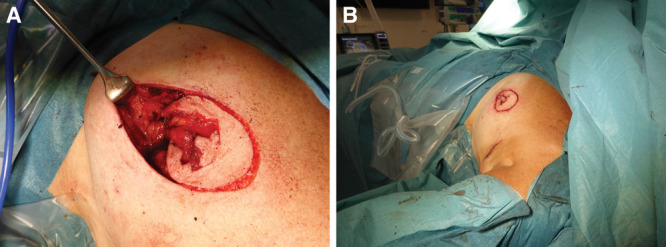
Several oncoplastic techniques have been proposed for subareolar breast cancer, some of which may require contralateral operation for symmetry, or more than one operation for delayed reconstruction of the nipple-areola complex (NAC). We herein developed a simple and effective oncoplastic approach following central quadrantectomy, aiming to achieve the following: (1) preservation of breast shape and contour for patients who are not accepting of a notably smaller breast or bilateral operation; (2) single procedure with advantages of single anesthetic and the ability to reconstruct a breast that has not yet been affected by radiation; (3) no autologous grafts with disadvantage of an extra donor site; (4) creation of natural neo-NAC with only incision within the region of the areola complex; and (5) maintaining long-term nipple projection. In this technique, the medial and lateral peri-areolar flap was advanced and rotated to restore partial neo-NAC, and to fill the defect after central tumor and NAC resection. The whole neo-NAC margin was created using the "round block" technique. Additionally, the nipple reconstruction was performed at the mitten of the neo-areola area using the C-V nipple flaps with an internal strut of rolled dermal grafts harvested from excised skin during the round block procedures. Lastly, a purse-string suture is placed in the outer skin margin for control of areola diameter and project. Six patients with central tumors of the breast were treated in this easily achieved approach. Patient satisfaction was noted as high, and the cosmetic results were evaluated as good to excellent.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Figures

Similar articles
-
Immediate Breast Reconstruction of a Nipple Areolar Lumpectomy Defect With the L-Flap Skin Paddle Breast Reduction Design and Contralateral Reduction Mammoplasty Symmetry Procedure: Optimizing the Oncoplastic Surgery Multispecialty Approach.Eplasty. 2017 Mar 31;17:e14. eCollection 2017. Eplasty. 2017. PMID: 28416989 Free PMC article.
-
Immediate reconstruction of the nipple/areola complex in oncoplastic surgery after central quadrantectomy.Ann Plast Surg. 2006 Dec;57(6):611-5. doi: 10.1097/01.sap.0000235444.51056.31. Ann Plast Surg. 2006. PMID: 17122544
-
Oncoplastic resection of retroareolar breast cancer: central quadrantectomy and reconstruction by local skin-glandular flap.J Egypt Natl Canc Inst. 2006 Dec;18(4):334-47. J Egypt Natl Canc Inst. 2006. PMID: 18301457 Clinical Trial.
-
Nipple-areola complex reconstruction.Gland Surg. 2014 Feb;3(1):35-42. doi: 10.3978/j.issn.2227-684X.2014.02.06. Gland Surg. 2014. PMID: 25083492 Free PMC article. Review.
-
Nipple Areola Complex Reconstruction: An 8-Year Experience With Modified Technique and Systematic Review.Eplasty. 2024 Jun 7;24:e36. eCollection 2024. Eplasty. 2024. PMID: 39224406 Free PMC article. Review.
References
-
- Recht A, Connolly JL, Schnitt SJ, et al. . Conservative surgery and radiation therapy for early breast cancer: Results, controversies, and unsolved problems. Semin Oncol. 1986;13:434–449. - PubMed
-
- Multon O, Bourgeois D, Validire P, et al. . [Breast cancers with central localization: Conservative treatment by tumorectomy with ablation of the areolar plaque]. Presse Med. 1997;26:988–994. - PubMed
-
- Clough KB, Cuminet J, Fitoussi A, et al. . Cosmetic sequelae after conservative treatment for breast cancer: Classification and results of surgical correction. Ann Plast Surg. 1998;41:471–481. - PubMed
-
- Bajaj AK, Kon PS, Oberg KC, et al. . Aesthetic outcomes in patients undergoing breast conservation therapy for the treatment of localized breast cancer. Plast Reconstr Surg. 2004;114:1442–1449. - PubMed
-
- Horiguchi J, Koibuchi Y, Iijima K, et al. . Local control by breast-conserving surgery with nipple resection. Anticancer Res. 2005;25:2957–2959. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources