

Review
doi: 10.1097/GOX.0000000000003431.
eCollection 2021 Feb.
Immediate Lymphatic Reconstruction: Technical Points and Literature Review
Affiliations
- PMID: 33680675
- PMCID: PMC7929616
- DOI: 10.1097/GOX.0000000000003431
Item in Clipboard
Review
Immediate Lymphatic Reconstruction: Technical Points and Literature Review
Plast Reconstr Surg Glob Open.
.
Abstract
Recent studies have provided evidence that lymphovenous bypass-microsurgical re-routing of divided lymphatics to an adjacent vein-performed at the time of lymph node dissection decreases the rate of lymphedema development. Immediate lymphatic reconstruction in this setting is technically demanding, and there is a paucity of literature describing the details of the surgical procedure. In this report, we review the literature supporting immediate lymphatic reconstruction and provide technical details to demystify the operation for surgeons who wish to provide this option to their patients.
Copyright © 2021 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Figures

ILR instruments and equipment setup.
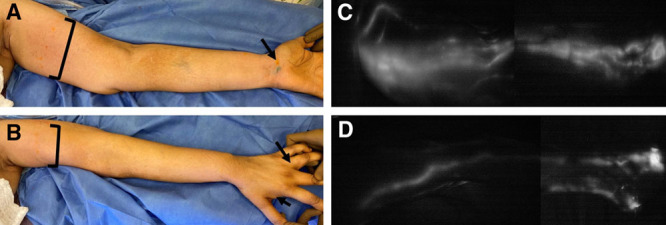
Upper extremity injection sites and ICG lymphangiogram with SPY-PHI. A, B, ICG is injected at 0.1 ml into the dermis of the first and third webspace, and the volar wrist. FITC is injected at 0.1 ml into the dermis of the first and third webspace, and the volar wrist. Additional FITC injections are done into the dermis across the medial upper arm (4–5 points with 0.1 ml each) and deeper, just above muscle fascia (1 point with 0.3 ml). C, D, ICG lymphangiogram showing the standard volar, radial, and ulnar lymphatic bundles merging at the upper inner arm.
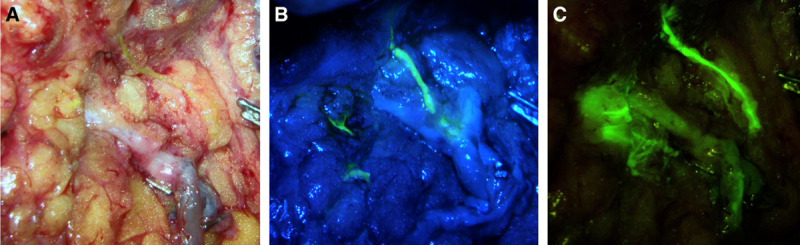
Visualization of lymphatic channels with FITC using the Mitaka microscope. A, With no filter, the lymphatic channel is slightly visible under white light. B, With a low-contrast fluorescence filter, there is visibility of non-fluorescent tissue and some fluorescence within the lymphatic channel. C, With a high-contrast fluorescence filter, there is poor visibility of non-fluorescent tissue, but excellent fluorescence seen within the lymphatic channel.
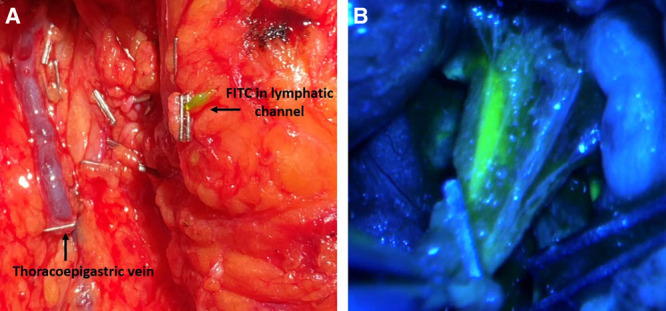
Lymphatic channel with FITC injected after ALND. A, Without the microscope, FITC is seen accumulating in the lymphatic channel up to the clip, dilating the lymphatic channel, on the right. Thoracoepigastric vein with clip on the left. B, Using the Mitaka microscope with a low-contrast fluorescence filter, there is visibility of surrounding tissue and fluorescence within the lymphatic channel.
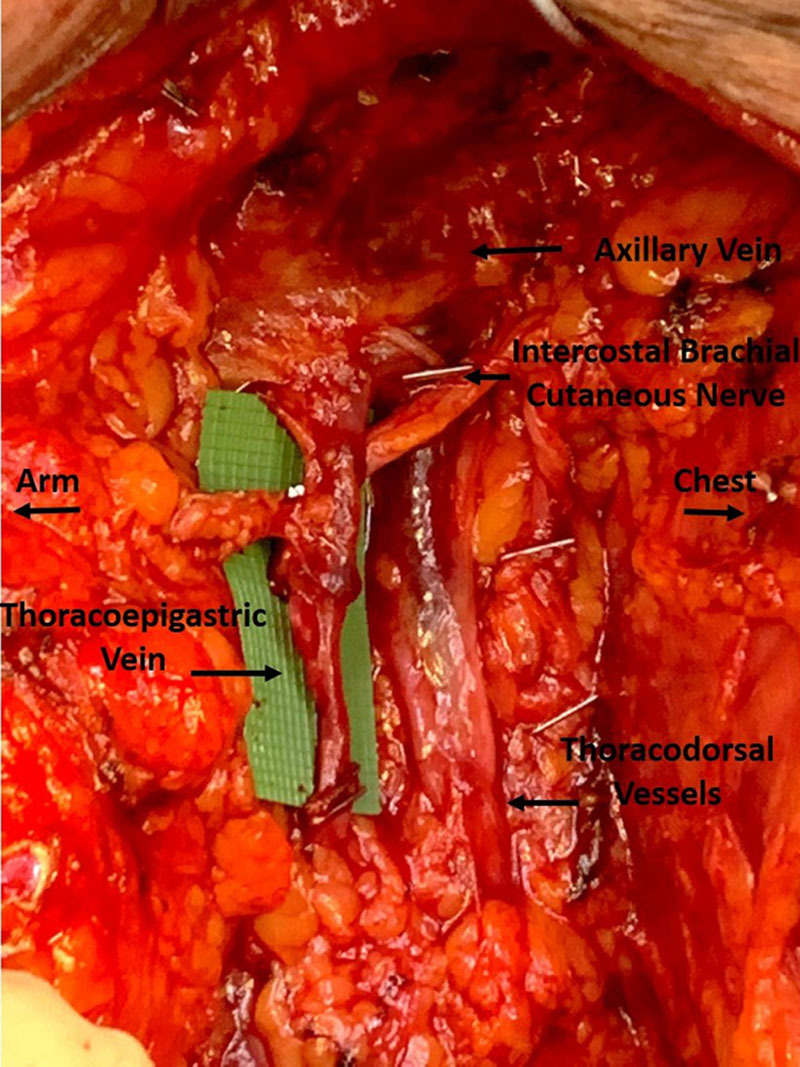
Thoracoepigastric (sometimes referred to as accessory) vein in axilla. The vein was dissected to a length of 6 cm, and there is a valve present at the midpoint. The intercostal brachial nerve is crossing posteriorly, and the thoracodorsal vessels are seen posterior to the thoracoepigastric vein.
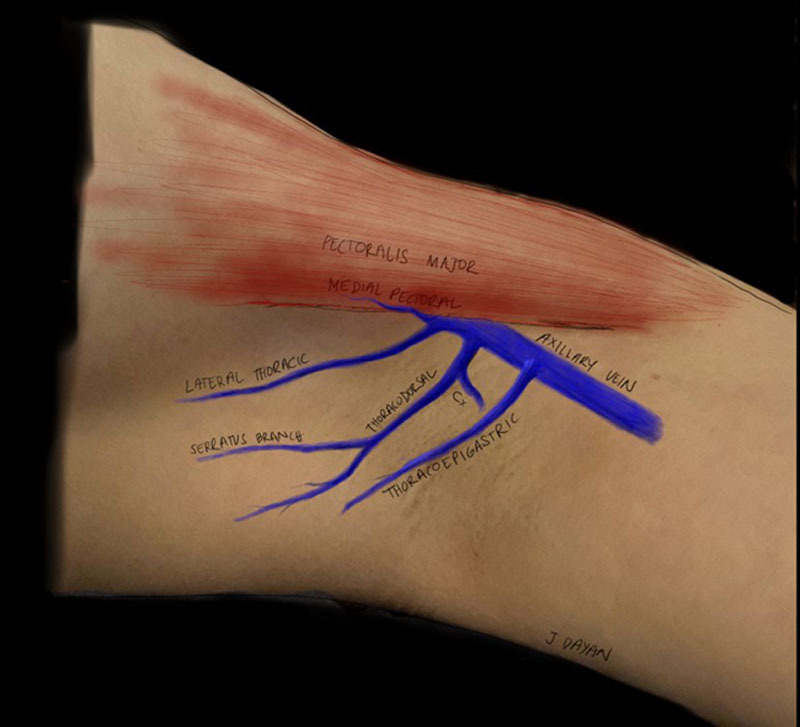
Alternative vein choices in the axilla. Illustrated are the medial pectoral vein running on the undersurface of the pectoralis major muscle, the lateral thoracic vein running on the lateral chest wall, the thoracodorsal vein and circumflex scapular vein (Cx) that are deeper in the axilla, and the thoracoepigastric vein (sometimes referred to as accessory) running more superficial (just below the clavipectoral fascia) to the thoracodorsal vessels.
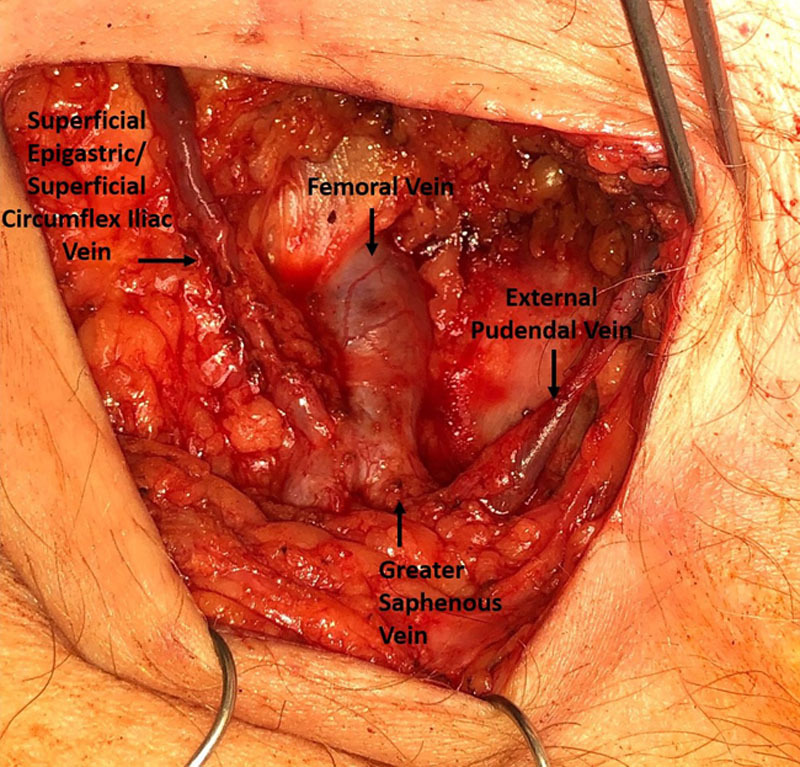
Vein choices in the groin. The superficial epigastric vein and superficial circumflex iliac vein course laterally from the femoral vein. The external pudendal vein courses medially.
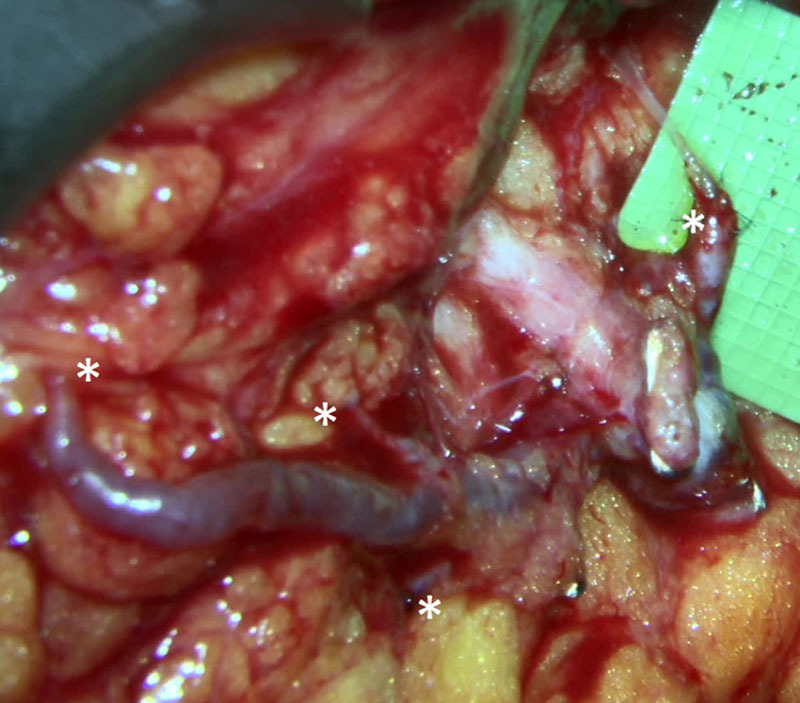
Thoracoepigastric vein with 4 branches and 4 separate anastomosis (*) of lymphatic channels at different locations and different depths in the axilla visualized through the Mitaka microscope (image is focused to deepest anastomosis; therefore, several proximal anastomosis appear blurred).
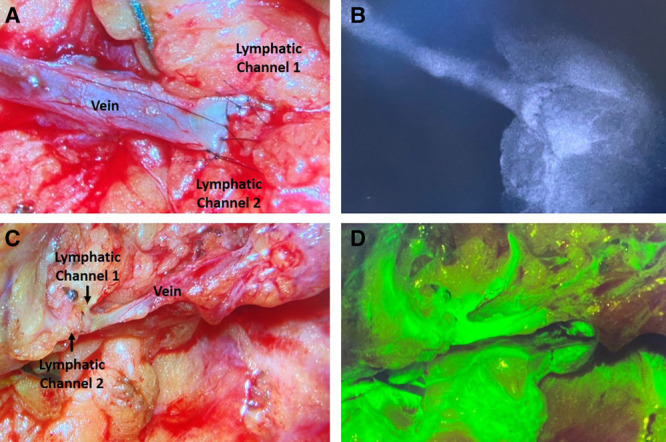
Verification of anastomotic patency using ICG and FITC. A, B, Two lymphatic channels anastomosed to the end of a vein with sutures closing the vein to itself centrally to prevent leakage. ICG seen flowing through the anastomosis, into the vein. C, D, Two lymphatic channels anastomosed to end of a vein branch. FITC seen flowing through the anastomosis, into the vein.
Similar articles
-
Lymphaticovenous Bypass for Immediate Lymphatic Reconstruction in Locoregional Advanced Melanoma Patients.J Reconstr Microsurg. 2020 May;36(4):247-252. doi: 10.1055/s-0039-3401829. Epub 2019 Dec 31. J Reconstr Microsurg. 2020. PMID: 31891946
-
Lymphatic Microsurgical Preventive Healing Approach (LYMPHA) for the prevention of secondary lymphedema.Breast J. 2020 Apr;26(4):721-724. doi: 10.1111/tbj.13667. Epub 2019 Oct 20. Breast J. 2020. PMID: 31631442
-
Lymphatic Microsurgical Preventing Healing Approach (LYMPHA) for Prevention of Breast Cancer-Related Lymphedema-a Preliminary Report.Indian J Surg Oncol. 2018 Sep;9(3):369-373. doi: 10.1007/s13193-018-0731-0. Epub 2018 Feb 17. Indian J Surg Oncol. 2018. PMID: 30288000 Free PMC article.
-
The treatment of lymphedema of the extremities with microsurgical lympho-venous anastomoses.Int Angiol. 1988 Oct-Dec;7(4):312-21. Int Angiol. 1988. PMID: 3072379 Review.
-
The lymphovenous microsurgical shunts for treatment of lymphedema of lower limbs: indications in 2011.Int Angiol. 2011 Dec;30(6):499-503. Int Angiol. 2011. PMID: 22233610 Review.
Cited by
-
A Prospective Study of Radiation Therapy After Immediate Lymphatic Reconstruction: Analysis of the Dosimetric Implications.Int J Radiat Oncol Biol Phys. 2023 Oct 1;117(2):446-451. doi: 10.1016/j.ijrobp.2023.04.027. Epub 2023 May 2. Int J Radiat Oncol Biol Phys. 2023. PMID: 37141983 Free PMC article.
-
MRI-CEUS fusion-guided lymphatic mapping as a preoperative strategy for lymphedema patients undergoing lymphaticovenous anastomosis surgery.J Vasc Surg Venous Lymphat Disord. 2024 Sep;12(5):101907. doi: 10.1016/j.jvsv.2024.101907. Epub 2024 May 15. J Vasc Surg Venous Lymphat Disord. 2024. PMID: 38759752 Free PMC article.
-
Effectiveness of the lymphatic microsurgical preventive healing approach for avoiding breast cancer-related arm lymphedema.Breast. 2025 Jul 14;83:104540. doi: 10.1016/j.breast.2025.104540. Online ahead of print. Breast. 2025. PMID: 40682911 Free PMC article.
-
Immediate lymphatic reconstruction: Outcomes of a single-institution pilot study.J Plast Reconstr Aesthet Surg. 2022 Mar;75(3):1261-1282. doi: 10.1016/j.bjps.2022.01.006. Epub 2022 Jan 19. J Plast Reconstr Aesthet Surg. 2022. PMID: 35094952 Free PMC article. No abstract available.
-
Immediate lymphatic reconstruction for the prevention of breast cancer-related lymphedema: an experience highlighting the importance of lymphatic anatomy.Plast Aesthet Res. 2023;10:23. doi: 10.20517/2347-9264.2022.100. Epub 2023 May 23. Plast Aesthet Res. 2023. PMID: 39640842 Free PMC article.
References
-
- Johnson AR, Asban A, Granoff MD, et al. . Is immediate lymphatic reconstruction cost-effective? Ann Surg. 2019. (E-pub ahead of print.) - PubMed
-
- Warren AG, Brorson H, Borud LJ, et al. . Lymphedema: A comprehensive review. Ann Plast Surg. 2007;59:464–472. - PubMed
-
- DiSipio T, Rye S, Newman B, et al. . Incidence of unilateral arm lymphoedema after breast cancer: A systematic review and meta-analysis. Lancet Oncol. 2013;14:500–515. - PubMed
-
- Petrek JA, Senie RT, Peters M, et al. . Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer. 2001;92:1368–1377. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources