

Latarjet Cerclage: The All-Arthroscopic Metal-Free Fixation
- PMID: 33680777
- PMCID: PMC7917201
- DOI: 10.1016/j.eats.2020.10.028
Latarjet Cerclage: The All-Arthroscopic Metal-Free Fixation
Abstract
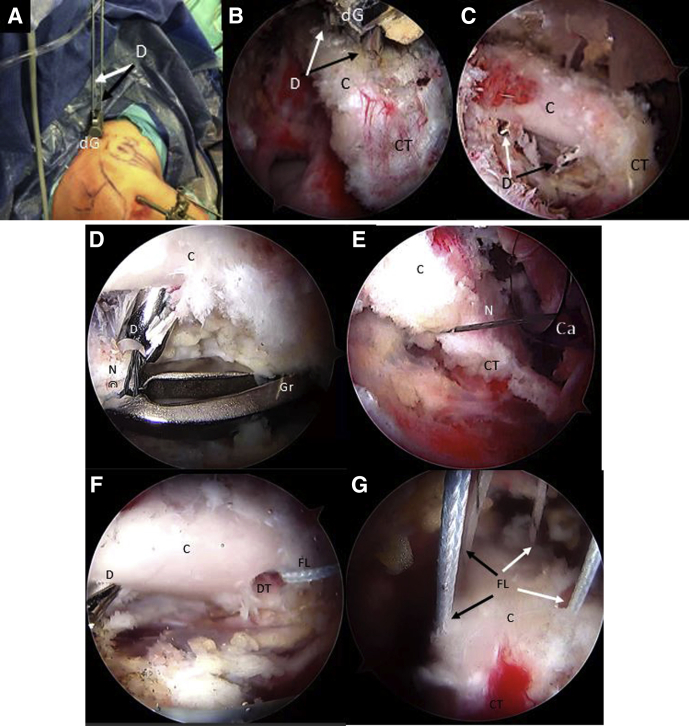
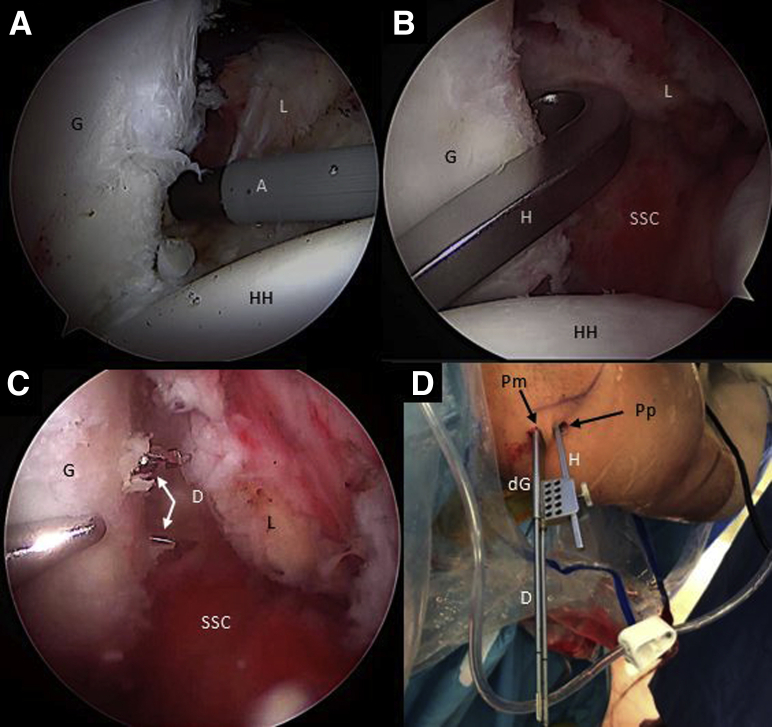
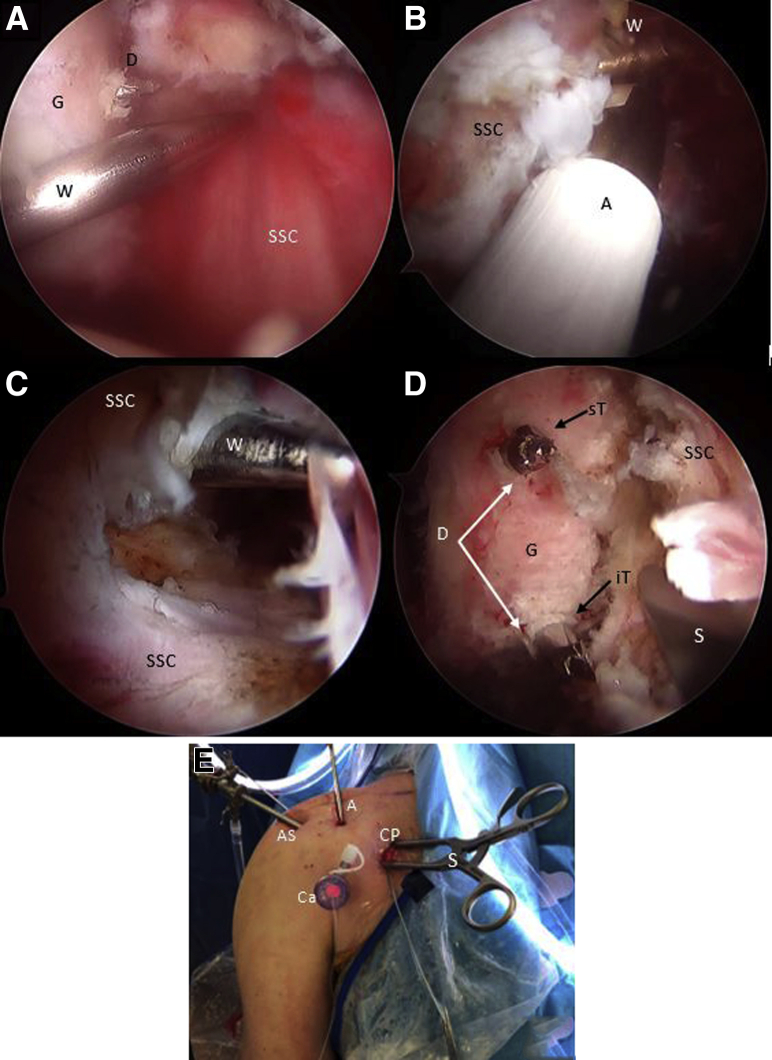
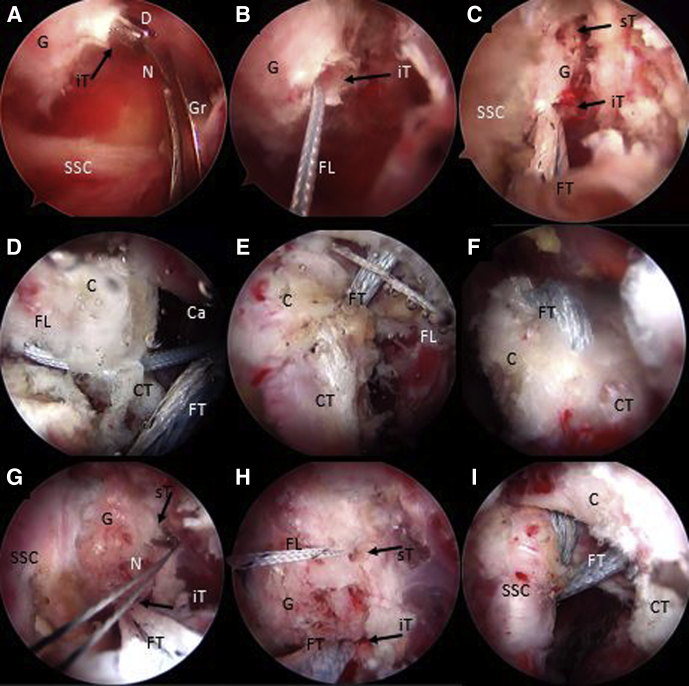
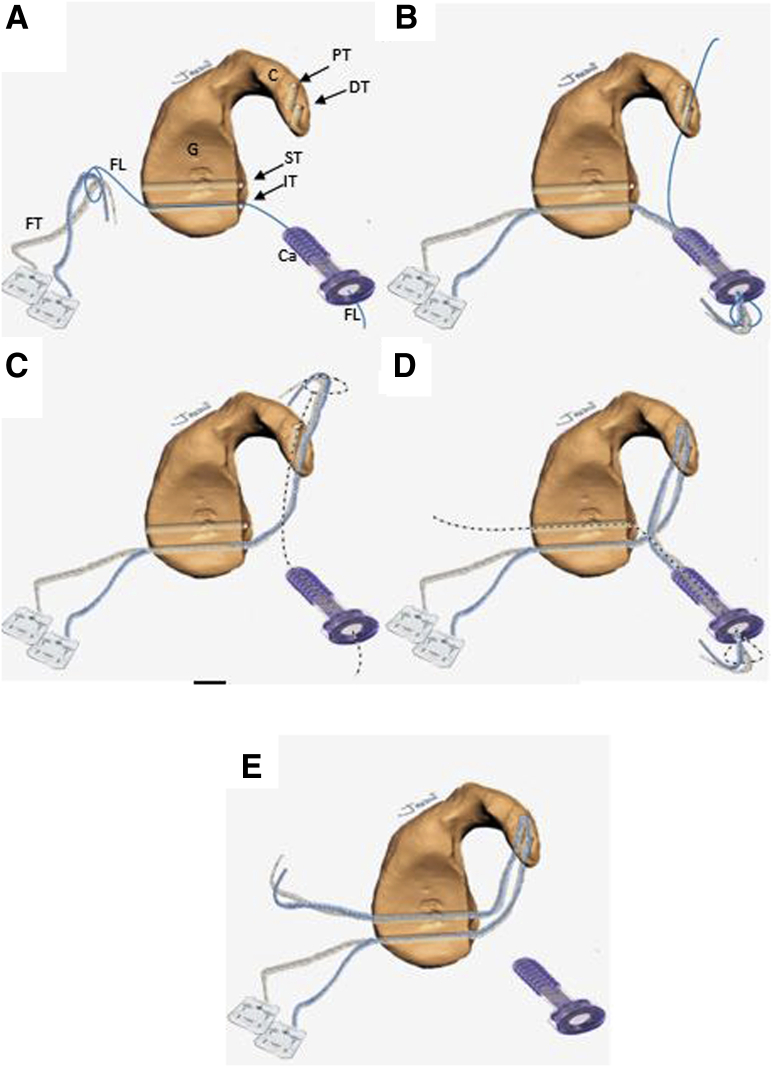
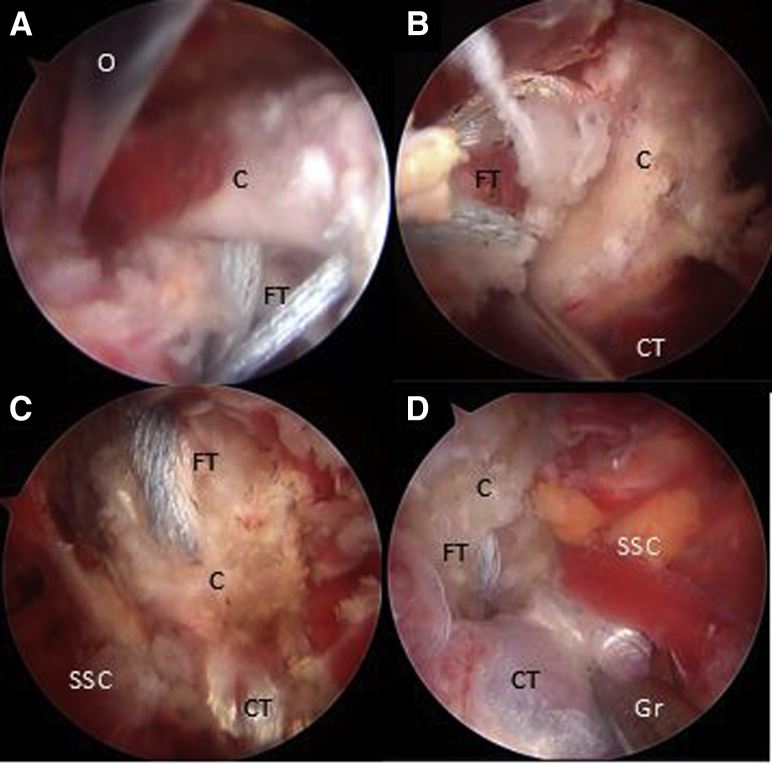
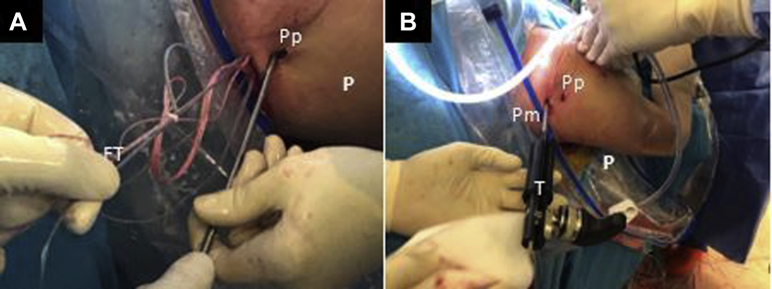
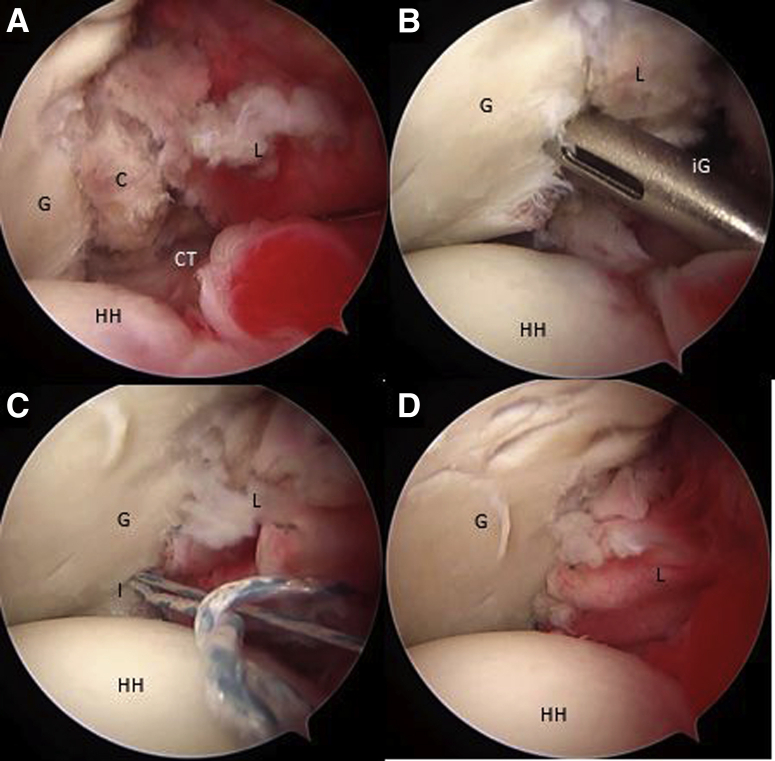
The Bristow-Latarjet procedure has been one of the most recognized procedures for the treatment of recurrent shoulder dislocation with anterior glenoid bone loss, revision surgery after failed Bankart repair, contact and collision sport injuries, and patients with a high risk of recurrence. Open and arthroscopic approaches have recently shown similar outcomes by several authors. However, complications related to metal implants, despite being low, are still a matter of concern. We describe an all-arthroscopic Latarjet technique with a metal-free fixation method using 2 ultra-high-strength sutures, creating a cerclage construct through 2.4mm glenoid and coracoid tunnels with a final capsulolabral complex reconstruction.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures

References
-
- Latarjet M. Treatment of recurrent dislocation of the shoulder. Lyon Chir. 1954;49:994–997. - PubMed
-
- Hurley E.T., Jamal M.S., Ali Z.S., Montgomery C., Pauzenberger L., Mullett H. Long-term outcomes of the Latarjet procedure for anterior shoulder instability: A systematic review of studies at 10-year follow-up. J Shoulder Elbow Surg. 2019;28:e33–e39. - PubMed
-
- Young A.A., Maia R., Berhouet J., Walch G. Open Latarjet procedure for management of bone loss in anterior instability of the glenohumeral joint. J Shoulder Elbow Surg. 2011;20:S61–S69. - PubMed
-
- Provencher M.T., Bhatia S., Ghodadra N.S. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg A. 2010;92(suppl 2):133–151. - PubMed
-
- Provencher M.T., Ferrari M.B., Sanchez G., Anavian J., Akamefula R., Lebus G.F. Current treatment options for glenohumeral instability and bone loss. JBJS Rev. 2017;5:1–11. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
