

An Unconventional View of T Cell Reconstitution After Allogeneic Hematopoietic Cell Transplantation
- PMID: 33680931
- PMCID: PMC7930482
- DOI: 10.3389/fonc.2020.608923
An Unconventional View of T Cell Reconstitution After Allogeneic Hematopoietic Cell Transplantation
Abstract
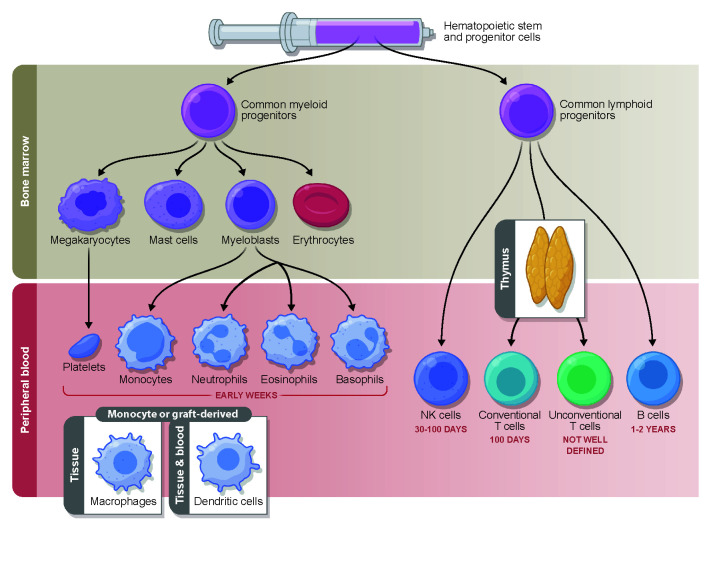
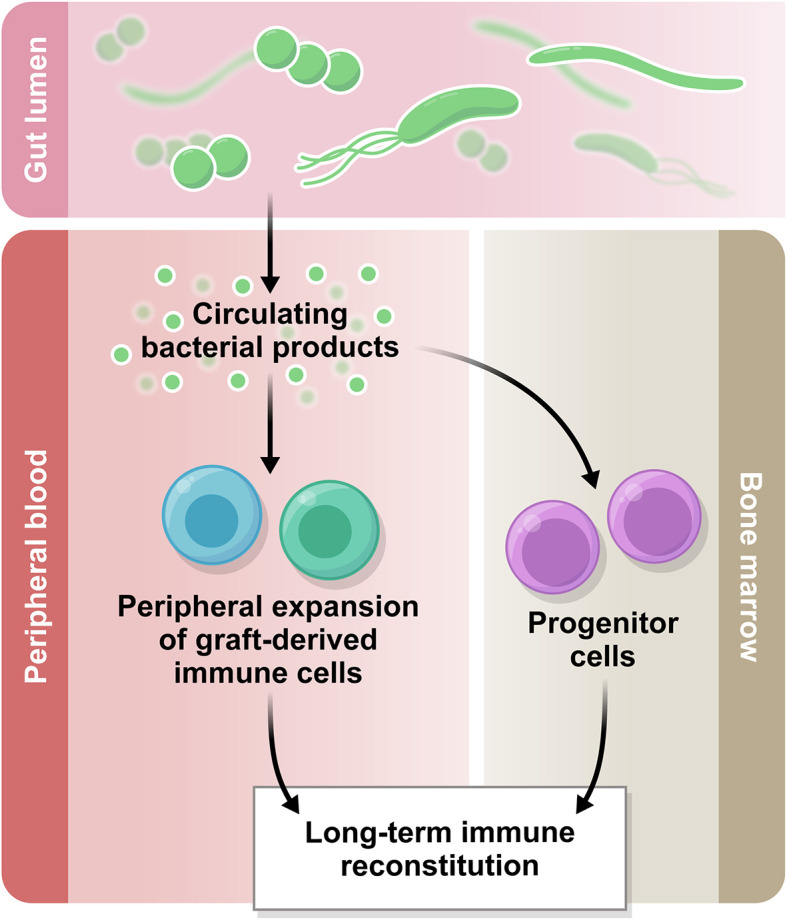
Allogeneic hematopoietic cell transplantation (allo-HCT) is performed as curative-intent therapy for hematologic malignancies and non-malignant hematologic, immunological and metabolic disorders, however, its broader implementation is limited by high rates of transplantation-related complications and a 2-year mortality that approaches 50%. Robust reconstitution of a functioning innate and adaptive immune system is a critical contributor to good long-term patient outcomes, primarily to prevent and overcome post-transplantation infectious complications and ensure adequate graft-versus-leukemia effects. There is increasing evidence that unconventional T cells may have an important immunomodulatory role after allo-HCT, which may be at least partially dependent on the post-transplantation intestinal microbiome. Here we discuss the role of immune reconstitution in allo-HCT outcome, focusing on unconventional T cells, specifically mucosal-associated invariant T (MAIT) cells, γδ (gd) T cells, and invariant NK T (iNKT) cells. We provide an overview of the mechanistic preclinical and associative clinical studies that have been performed. We also discuss the emerging role of the intestinal microbiome with regard to hematopoietic function and overall immune reconstitution.
Keywords: allogeneic transplantation; immune reconstitution; invariant NK T (iNKT) cells; microbiome; mucosal invariant T cells (MAIT) cells; unconventional T cells; γδ T cells.
Copyright © 2021 Andrlová, van den Brink and Markey.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources