

The "TIDE"-Algorithm for the Weaning of Patients With Cardiogenic Shock and Temporarily Mechanical Left Ventricular Support With Impella Devices. A Cardiovascular Physiology-Based Approach
- PMID: 33681302
- PMCID: PMC7933542
- DOI: 10.3389/fcvm.2021.563484
The "TIDE"-Algorithm for the Weaning of Patients With Cardiogenic Shock and Temporarily Mechanical Left Ventricular Support With Impella Devices. A Cardiovascular Physiology-Based Approach
Abstract
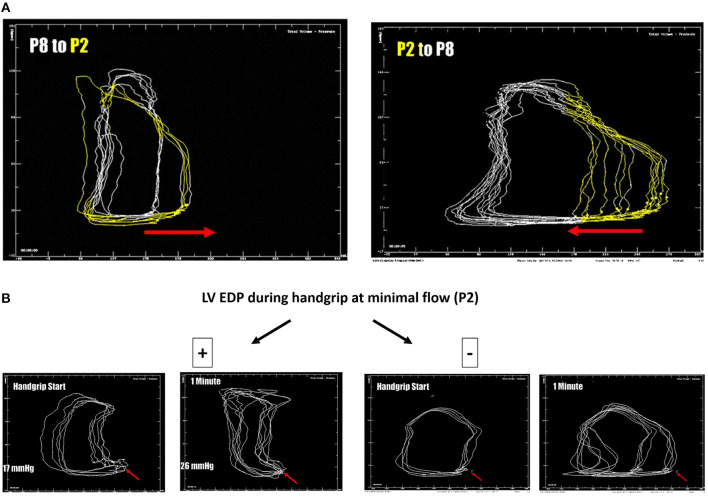
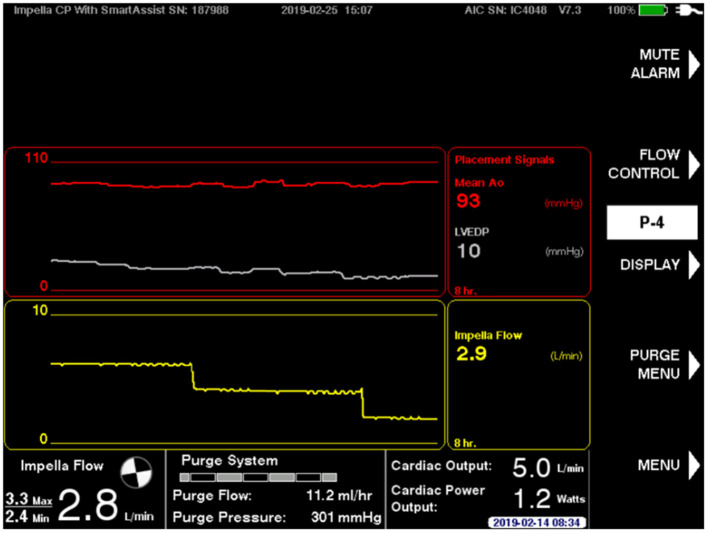
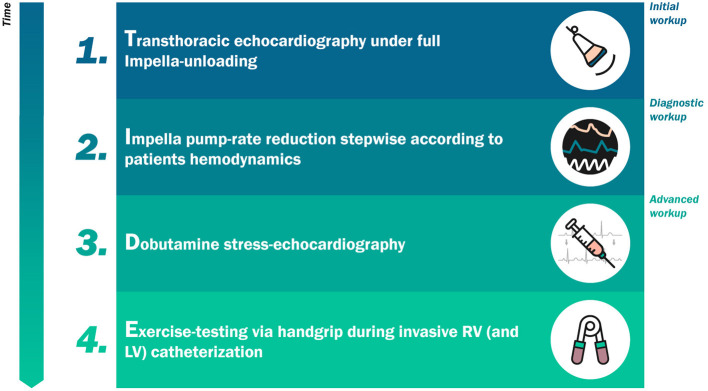
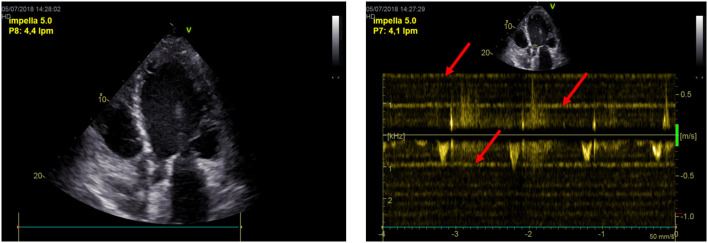
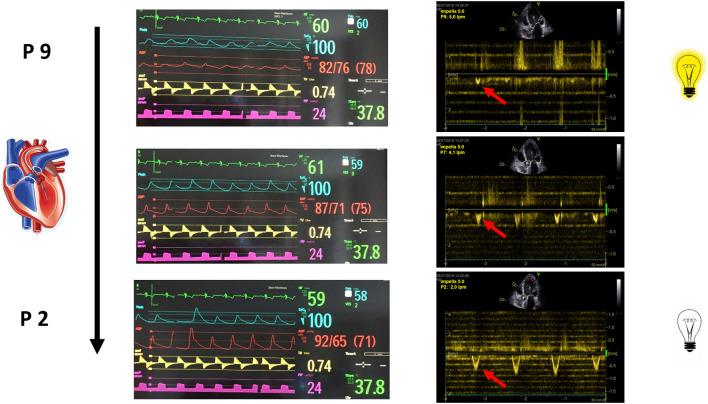
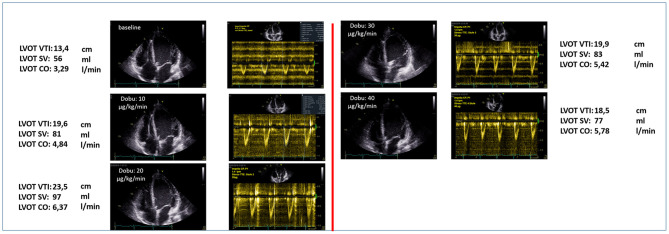
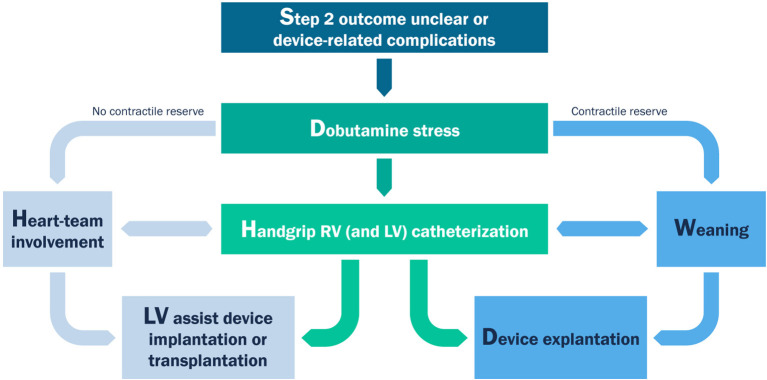
Objectives: Mechanical circulatory support (MCS) is often required to stabilize therapy-refractory cardiogenic shock patients. Left ventricular (LV) unloading by mechanical ventricular support (MVS) via percutaneous devices, such as with Impella® axial pumps, alone or in combination with extracorporeal life support (ECLS, ECMELLA approach), has emerged as a potential clinical breakthrough in the field. While the weaning from MCS is essentially based on the evaluation of circulatory stability of patients, weaning from MVS holds a higher complexity, being dependent on bi-ventricular function and its adaption to load. As a result of this, weaning from MVS is mostly performed in the absence of established algorithms. MVS via Impella is applied in several cardiogenic shock etiologies, such as acute myocardial infarction (support over days) or acute fulminant myocarditis (prolonged support over weeks, PROPELLA). The time point of weaning from Impella in these cohorts of patients remains unclear. We here propose a novel cardiovascular physiology-based weaning algorithm for MVS. Methods: The proposed algorithm is based on the experience gathered at our center undergoing an Impella weaning between 2017 and 2020. Before undertaking a weaning process, patients must had been ECMO-free, afebrile, and euvolemic, with hemodynamic stability guaranteed in the absence of any inotropic support. The algorithm consists of 4 steps according to the acronym TIDE: (i) Transthoracic echocardiography under full Impella-unloading; (ii) Impella rate reduction in single 8-24 h-steps according to patients hemodynamics (blood pressure, heart rate, and ScVO2), including a daily echocardiographic assessment at minimal flow (P2); (iii) Dobutamine stress-echocardiography; (iv) Right heart catheterization at rest and during Exercise-testing via handgrip. We here present clinical and hemodynamic data (including LV conductance data) from paradigmatic weaning protocols of awake patients admitted to our intensive care unit with cardiogenic shock. We discuss the clinical consequences of the TIDE algorithm, leading to either a bridge-to-recovery, or to a bridge-to-permanent LV assist device (LVAD) and/or transplantation. With this protocol we were able to wean 74.2% of the investigated patients successfully. 25.8% showed a permanent weaning failure and became LVAD candidates. Conclusions: The proposed novel cardiovascular physiology-based weaning algorithm is based on the characterization of the extent and sustainment of LV unloading reached during hospitalization in patients with cardiogenic shock undergoing MVS with Impella in our center. Prospective studies are needed to validate the algorithm.
Keywords: Impella; cardiogenic shock; conductance catheter; mechanical circulatory support; pressure-volume; weaning algorithm.
Copyright © 2021 Tschöpe, Spillmann, Potapov, Faragli, Rapis, Nelki, Post, Schmidt and Alogna.
Conflict of interest statement
CT, FS, and GS received honoraria for talks from Abiomed. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Goldberg RJ, Makam RC, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-Long trends (2001–2011) in the incidence and hospital death rates associated with the in-hospital development of cardiogenic shock after acute myocardial infarction. Circ Cardiovasc Qual Outcomes. (2016) 9:117–25. 10.1161/CIRCOUTCOMES.115.002359 - DOI - PMC - PubMed
-
- Aissaoui N, Puymirat E, Tabone X, Charbonnier B, Schiele F, Lefevre T, et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction: a report from the USIK 1995, USIC 2000, and FAST-MI French nationwide registries. Eur Heart J. (2012) 33:2535–43. 10.1093/eurheartj/ehs264 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials