

Locked pubis symphysis in a skeletally immature patient, a case report
- PMID: 33681444
- PMCID: PMC7918673
- DOI: 10.1016/j.tcr.2021.100441
Locked pubis symphysis in a skeletally immature patient, a case report
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.Trauma Case Rep. 2023 Feb 17;45:100794. doi: 10.1016/j.tcr.2023.100794. eCollection 2023 Jun. Trauma Case Rep. 2023. PMID: 37234575 Free PMC article.
-
Erratum regarding missing patient consent statement in previously published articles.Trauma Case Rep. 2023 Mar 1;45:100811. doi: 10.1016/j.tcr.2023.100811. eCollection 2023 Jun. Trauma Case Rep. 2023. PMID: 37234579 Free PMC article.
Abstract
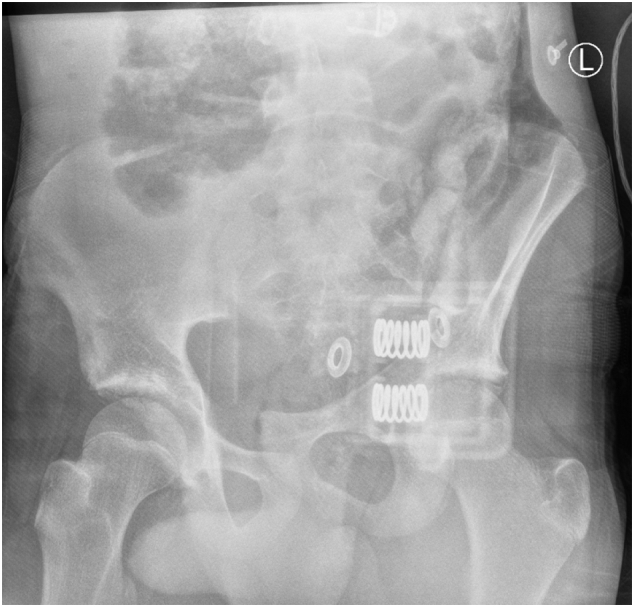
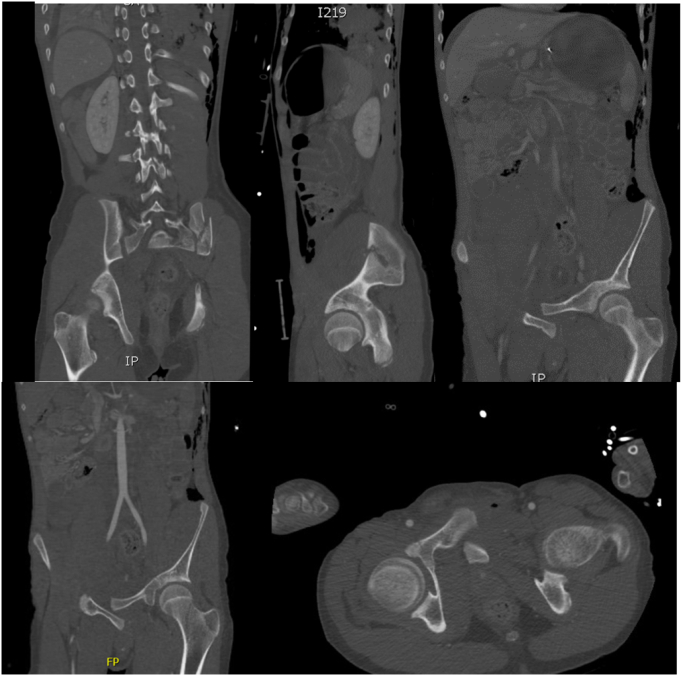
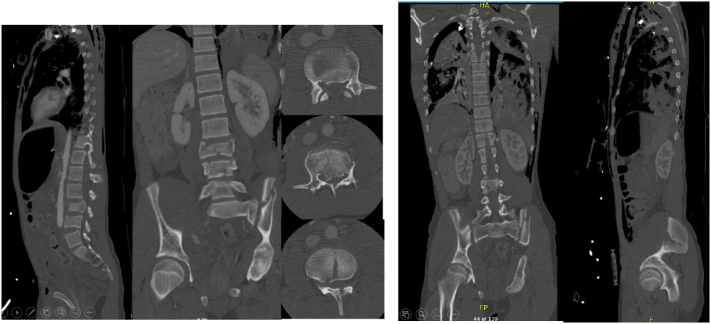
Background: Locked symphysis pubis is an exceedingly rare pelvic injury especially in the paediatric population. This study is the first to describe this fracture in a skeletally immature patient.
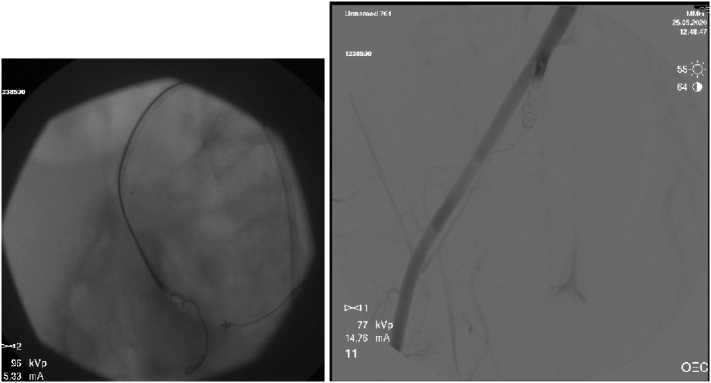
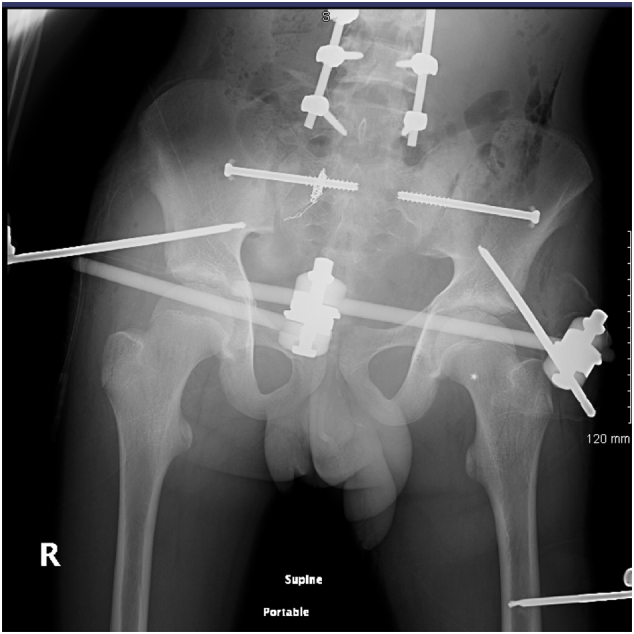
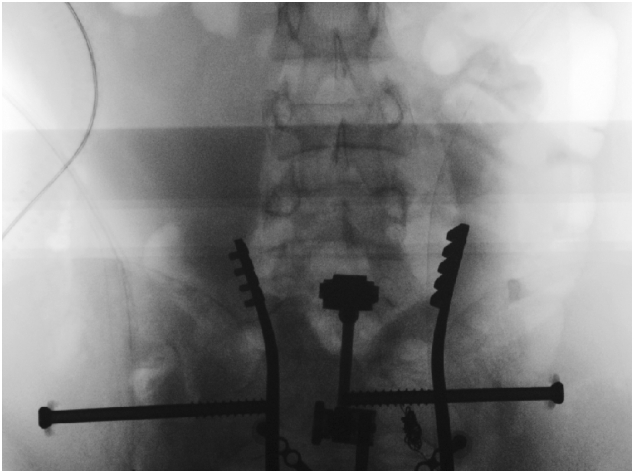
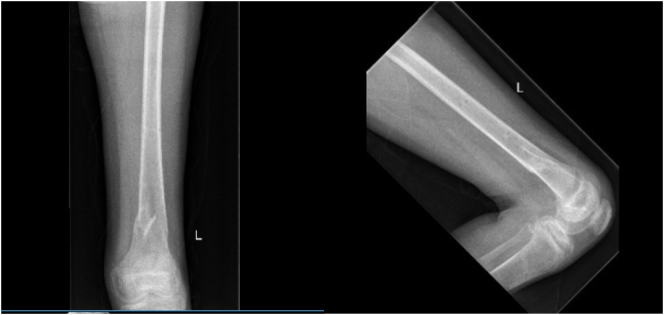
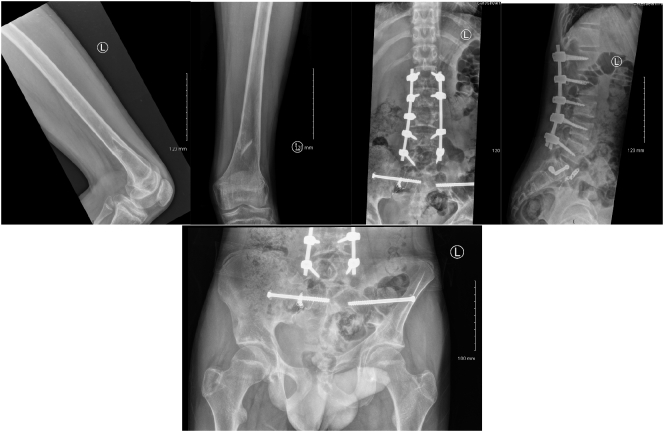
Case report: We report the case of a fifteen year old boy who presented to the Emergency Department (ED) after being involved in a farming injury with a left lateral compression pelvic trauma. He sustained Locked Symphysis Pubis (LSP) and internal pelvic bleeding from the right Internal Iliac Artery (IIA). He was treated successfully by selective embolization of the ILA followed by closed reduction of the LSP and percutaneous fixation of the SI joint.
Conclusion: Locked symphysis pubis in the paediatric population is an exceedingly rare injury among lateral compression type pelvic fractures. Careful assessment and preoperative management planning are encouraged. Open packing of the pelvis in case of internal bleeding should be avoided in paediatric patients, only selective embolization is advocated. Closed reduction of the LSP by using the external fixator as a lever arm for reduction followed by percutaneous fixation of the SI joint. Moreover, changing the patient position to prone position followed by posterior lumbar spine stabilisation is our preferred method of treatment.
Keywords: Case report; Locked pubic symphysis; Overlapped pubic symphysis; Pelvic fracture; Spine fracture.
© 2021 The Author(s).
Figures

References
-
- E G.W. Dislocations of the os coxae. Am. J. Surg. 1952;83:300–307. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
