

Early Allograft Dysfunction Increases Hospital Associated Costs After Liver Transplantation-A Propensity Score-Matched Analysis
- PMID: 33681684
- PMCID: PMC7917275
- DOI: 10.1002/hep4.1651
Early Allograft Dysfunction Increases Hospital Associated Costs After Liver Transplantation-A Propensity Score-Matched Analysis
Abstract
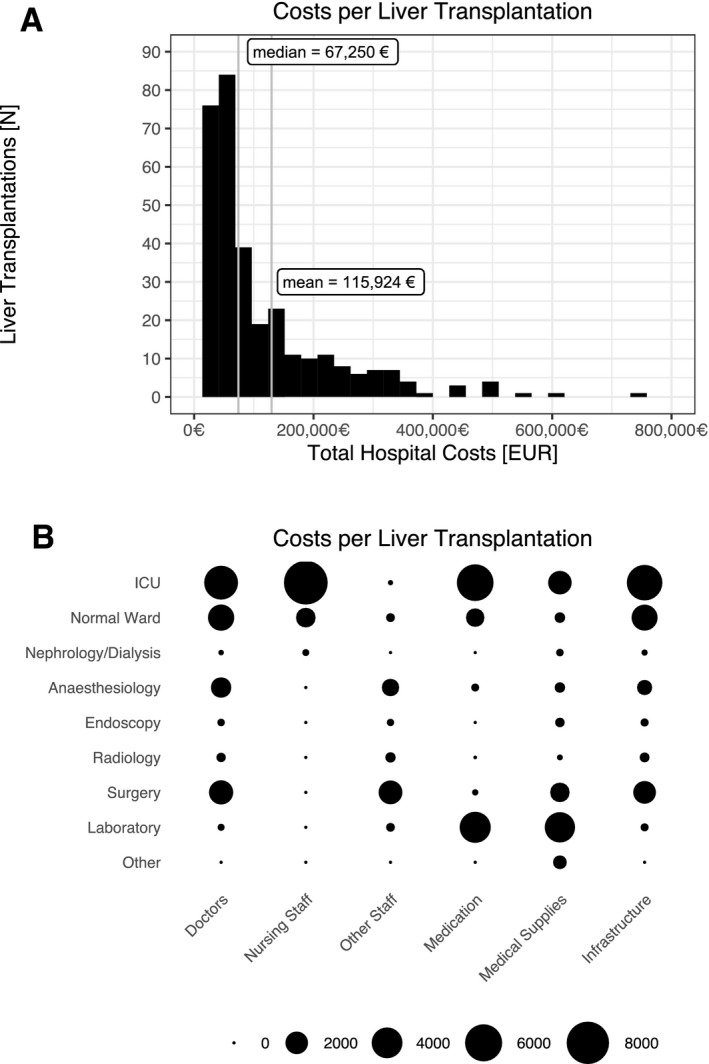
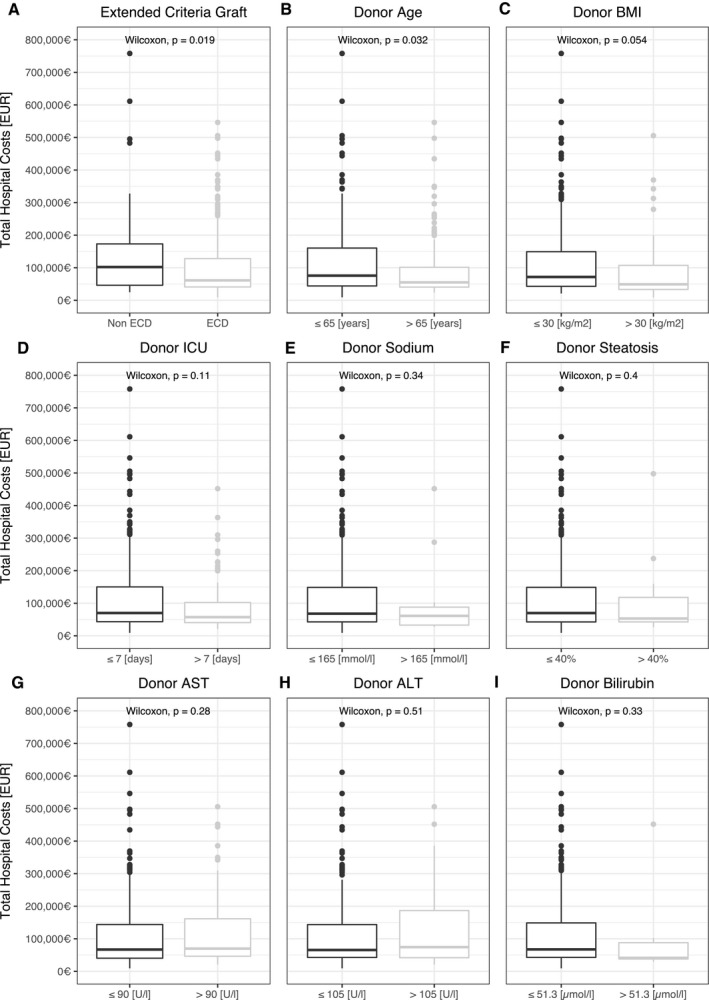
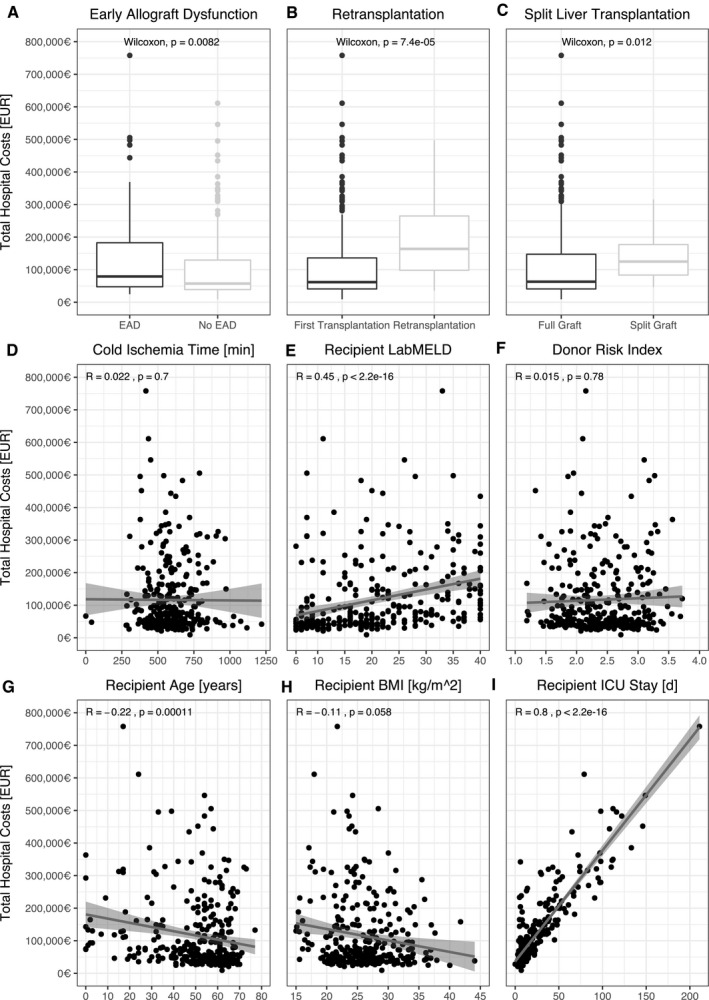
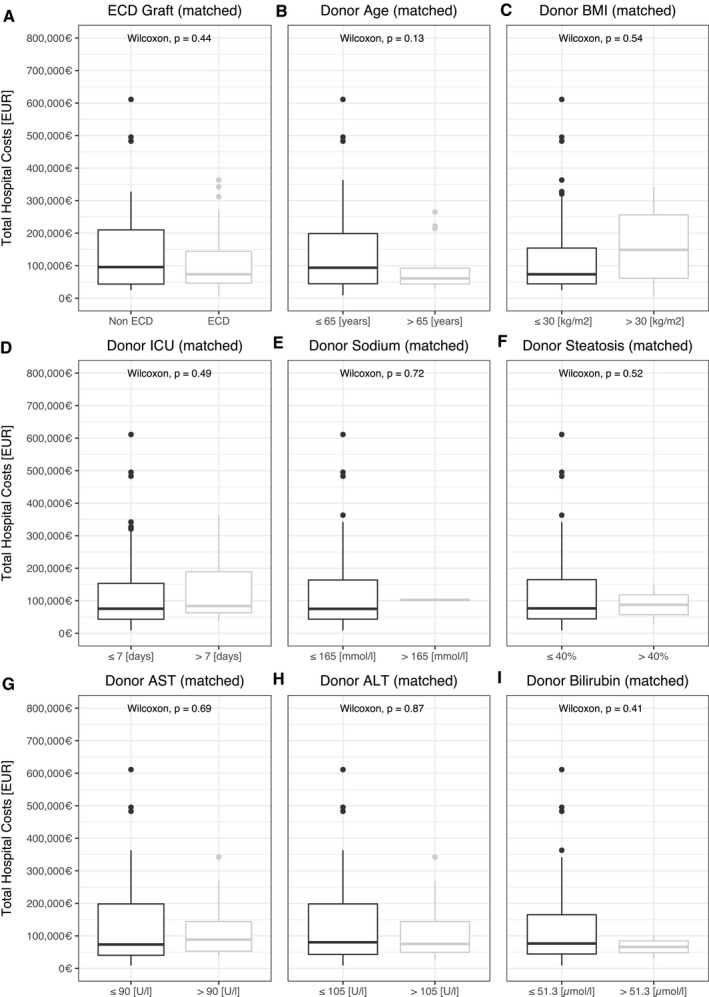
Concepts to ameliorate the continued mismatch between demand for liver allografts and supply include the acceptance of allografts that meet extended donor criteria (ECD). ECD grafts are generally associated with an increased rate of complications such as early allograft dysfunction (EAD). The costs of liver transplantation for the health care system with respect to specific risk factors remain unclear and are subject to change. We analyzed 317 liver transplant recipients from 2013 to 2018 for outcome after liver transplantation and hospital costs in a German transplant center. In our study period, 1-year survival after transplantation was 80.1% (95% confidence interval: 75.8%-84.6%) and median hospital stay was 33 days (interquartile rage: 24), with mean hospital costs of €115,924 (SD €113,347). There was a positive correlation between costs and laboratory Model for End-Stage Liver Disease score (rs = 0.48, P < 0.001), and the development of EAD increased hospital costs by €26,229. ECD grafts were not associated with a higher risk of EAD in our cohort. When adjusting for recipient-associated risk factors such as laboratory Model for End-Stage Liver Disease score, recipient age, and split liver transplantation with propensity score matching, only EAD and cold ischemia increased total costs. Conclusion: Our data show that EAD leads to significantly higher hospital costs for liver transplantation, which are primarily attributed to recipient health status. Strategies to reduce the incidence of EAD are needed to control costs in liver transplantation.
© 2020 The Authors. Hepatology Communications published by Wiley Periodicals LLC on behalf of the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Smartphone Apps to Stratify the Risk of Early Allograft Failure Are Just the Beginning for Next-Generation Outcome Prediction in Transplantation Medicine.Hepatol Commun. 2022 Jan;6(1):249. doi: 10.1002/hep4.1755. Epub 2021 Jun 21. Hepatol Commun. 2022. PMID: 34558813 Free PMC article. No abstract available.
-
Availability of a Web and Smartphone Application to Stratify the Risk of of Early Allograft Failure Requiring Liver Retransplantation.Hepatol Commun. 2022 Jan;6(1):247-248. doi: 10.1002/hep4.1754. Epub 2021 Jun 22. Hepatol Commun. 2022. PMID: 34558843 Free PMC article.
References
-
- Jackson KR, Motter JD, Haugen CE, Holscher C, Long JJ, Massie AB, et al. Temporal trends in utilization and outcomes of steatotic donor livers in the United States. Am J Transplant 2020;20:855‐863. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
