

Different effects of morning and nocturnal hypertension on target organ damage in chronic kidney disease
- PMID: 33682307
- PMCID: PMC8678691
- DOI: 10.1111/jch.14234
Different effects of morning and nocturnal hypertension on target organ damage in chronic kidney disease
Abstract
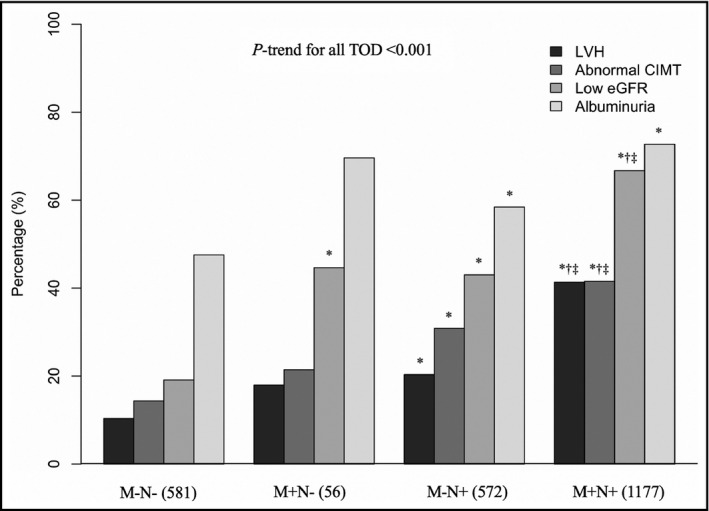
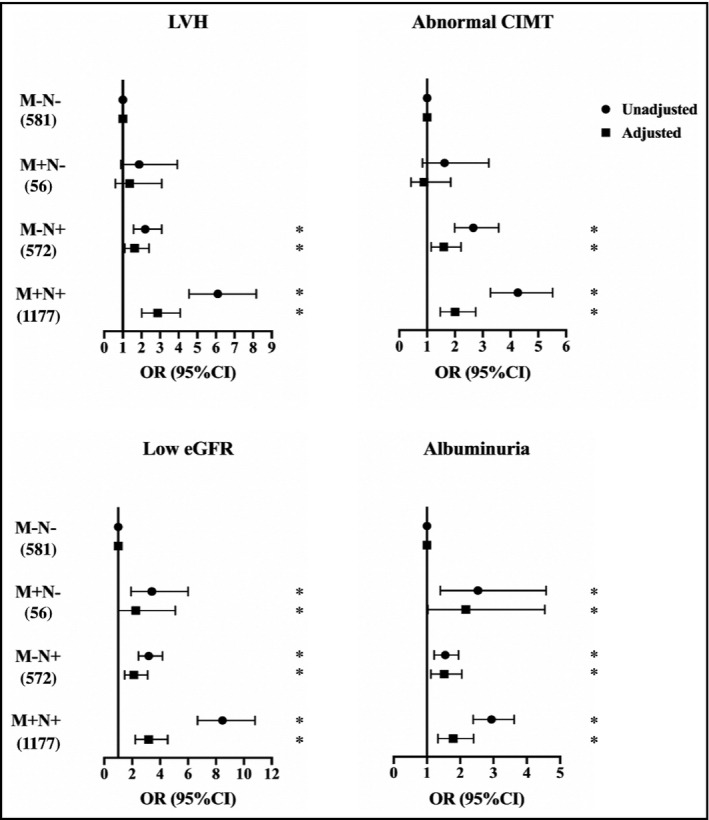
Both morning hypertension (MH) and nocturnal hypertension (NH) are associated with severe target organ damage in patients with chronic kidney disease (CKD). However, the isolated or combined effects of MH and NH on target organ damage are less well-defined. A cross-sectional study was conducted among 2386 non-dialysis CKD patients with ambulatory blood pressure monitoring. The authors categorized patients into four groups based on the presence or absence of MH and NH. Multivariate logistic analyses were used to evaluate the correlation between hypertension subtypes and target organ damage, including left ventricular hypertrophy (LVH), abnormal carotid intima-media thickness (CIMT), low estimated glomerular filtration rate (eGFR), and albuminuria. The percentages of isolated MH, isolated NH, and combined MH and NH were 2.3%, 24.0%, and 49.3%, respectively. Compared to patients without MH and NH, isolated MH was only related to low eGFR (2.26 [95% confidence interval: 1.00-5.09]) and albuminuria (2.17 [95% CI: 1.03-4.54]). Meanwhile, combined MH and NH group compared to the group without MH and NH had a higher risk of LVH (2.87 [95% CI: 2.01-4.09]), abnormal CIMT (2.01 [95% CI: 1.47-2.75]), low eGFR (3.18 [95% CI: 2.23-4.54]), and albuminuria (1.79 [95% CI: 1.33-2.40]), even in patients without daytime hypertension. The risk of cardiovascular and renal damage was also observed in the isolated NH group. In conclusion, morning hypertension is associated with kidney dysfunction and has combined effects with nocturnal hypertension on cardiovascular damage in chronic kidney disease patients.
Keywords: ambulatory blood pressure monitoring; chronic kidney disease; morning hypertension; nocturnal hypertension; target organ damage.
© 2021 The Authors. The Journal of Clinical Hypertension published by Wiley Periodicals LLC.
Conflict of interest statement
None.
Figures
Similar articles
-
Nocturnal pulse rate correlated with ambulatory blood pressure and target organ damage in patients with chronic kidney disease.J Clin Hypertens (Greenwich). 2019 Jan;21(1):77-87. doi: 10.1111/jch.13438. Epub 2018 Dec 31. J Clin Hypertens (Greenwich). 2019. PMID: 30597750 Free PMC article.
-
Association between short-term blood pressure variability and target organ damage in non-dialysis patients with chronic kidney disease.BMC Nephrol. 2024 Mar 21;25(1):111. doi: 10.1186/s12882-024-03541-x. BMC Nephrol. 2024. PMID: 38515022 Free PMC article.
-
High prevalence of isolated nocturnal hypertension in Chinese patients with chronic kidney disease.J Am Heart Assoc. 2015 Jun 18;4(6):e002025. doi: 10.1161/JAHA.115.002025. J Am Heart Assoc. 2015. PMID: 26089178 Free PMC article.
-
Hypertension and Organ Damage in Women.High Blood Press Cardiovasc Prev. 2018 Sep;25(3):245-252. doi: 10.1007/s40292-018-0265-0. Epub 2018 Jun 26. High Blood Press Cardiovasc Prev. 2018. PMID: 29943358 Review.
-
Subclinical Kidney Damage in Hypertensive Patients: A Renal Window Opened on the Cardiovascular System. Focus on Microalbuminuria.Adv Exp Med Biol. 2017;956:279-306. doi: 10.1007/5584_2016_85. Adv Exp Med Biol. 2017. PMID: 27873229 Review.
Cited by
-
Association of Nighttime Masked Uncontrolled Hypertension With Left Ventricular Hypertrophy and Kidney Function Among Patients with Chronic Kidney Disease Not Receiving Dialysis.JAMA Netw Open. 2022 May 2;5(5):e2214460. doi: 10.1001/jamanetworkopen.2022.14460. JAMA Netw Open. 2022. PMID: 35616936 Free PMC article.
-
Prognostic Effect of Masked Morning Hypertension in Chinese Inpatients With Non-dialysis Chronic Kidney Disease: A Multicenter Retrospective Study.Am J Hypertens. 2024 Jul 15;37(8):621-630. doi: 10.1093/ajh/hpae044. Am J Hypertens. 2024. PMID: 38625716 Free PMC article.
References
-
- Gansevoort RT, Correa‐Rotter R, Hemmelgarn BR, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339‐352. - PubMed
-
- Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713‐735. - PubMed
-
- Huang Q‐F, Hoshide S, Cheng H‐M, et al. Management of hypertension in patients with chronic kidney disease in Asia. Curr Hypertens Rev. 2016;12(3):181‐185. - PubMed
-
- Simon A, Megnien JL, Chironi G. The value of carotid intima‐media thickness for predicting cardiovascular risk. Arterioscler Thromb Vasc Biol. 2010;30(2):182‐185. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
