

Dynamic Changes in the Nasal Microbiome Associated With Disease Activity in Patients With Granulomatosis With Polyangiitis
- PMID: 33682371
- PMCID: PMC8403103
- DOI: 10.1002/art.41723
Dynamic Changes in the Nasal Microbiome Associated With Disease Activity in Patients With Granulomatosis With Polyangiitis
Abstract
Objective: Little is known about temporal changes in nasal bacteria in granulomatosis with polyangiitis (GPA). This study was undertaken to examine longitudinal changes in the nasal microbiome in association with relapse in GPA patients.
Methods: Bacterial 16S ribosomal RNA gene sequencing was performed on nasal swabs from 19 patients with GPA who were followed up longitudinally for a total of 78 visits, including 9 patients who experienced a relapse and 10 patients who remained in remission. Relative abundance of bacteria and ratios between bacteria were examined. Generalized estimating equation models were used to evaluate the association between bacterial composition and 1) disease activity and 2) levels of antineutrophil cytoplasmic antibody (ANCA) with specificity for proteinase 3 (PR3), adjusted for medication.
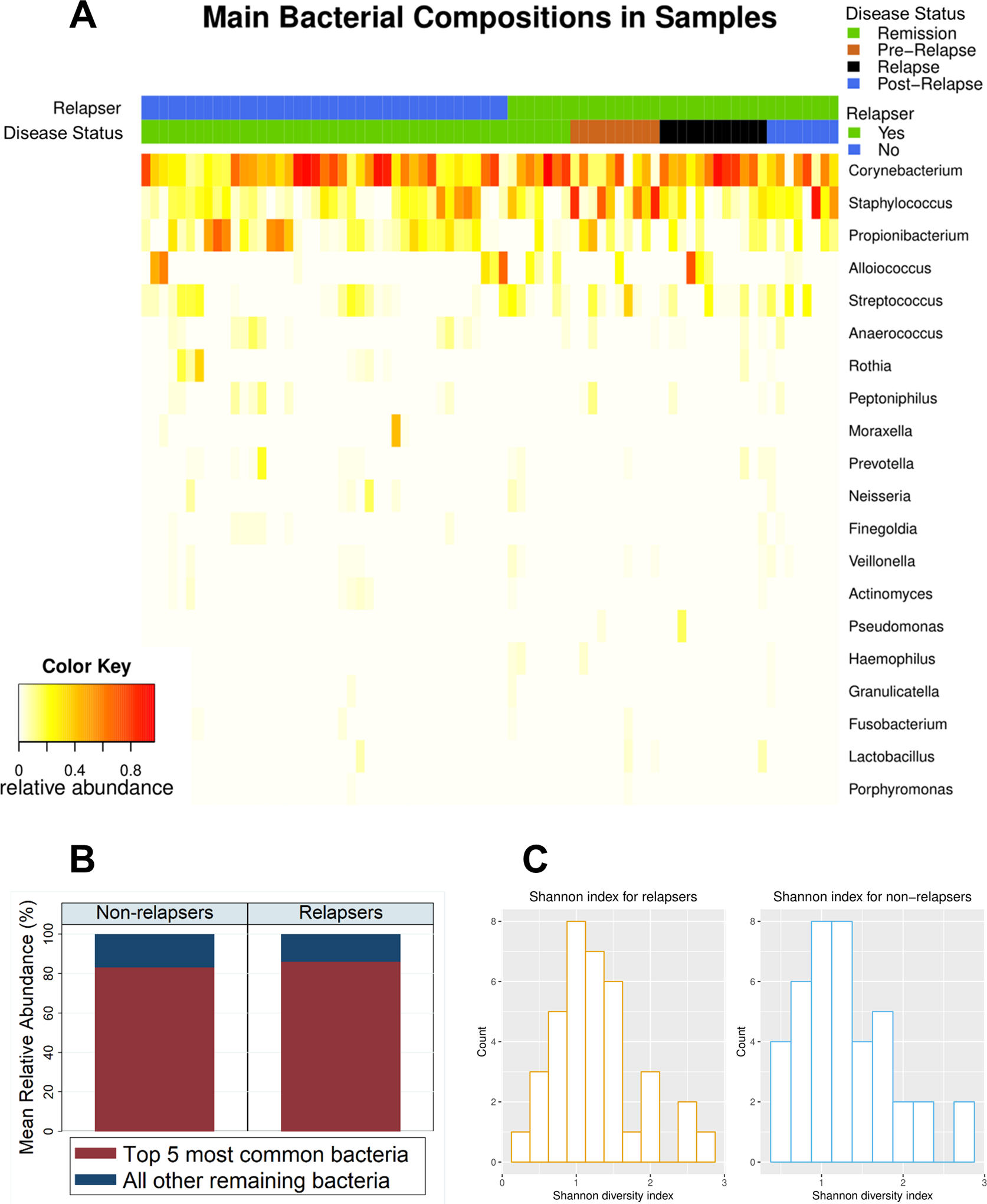
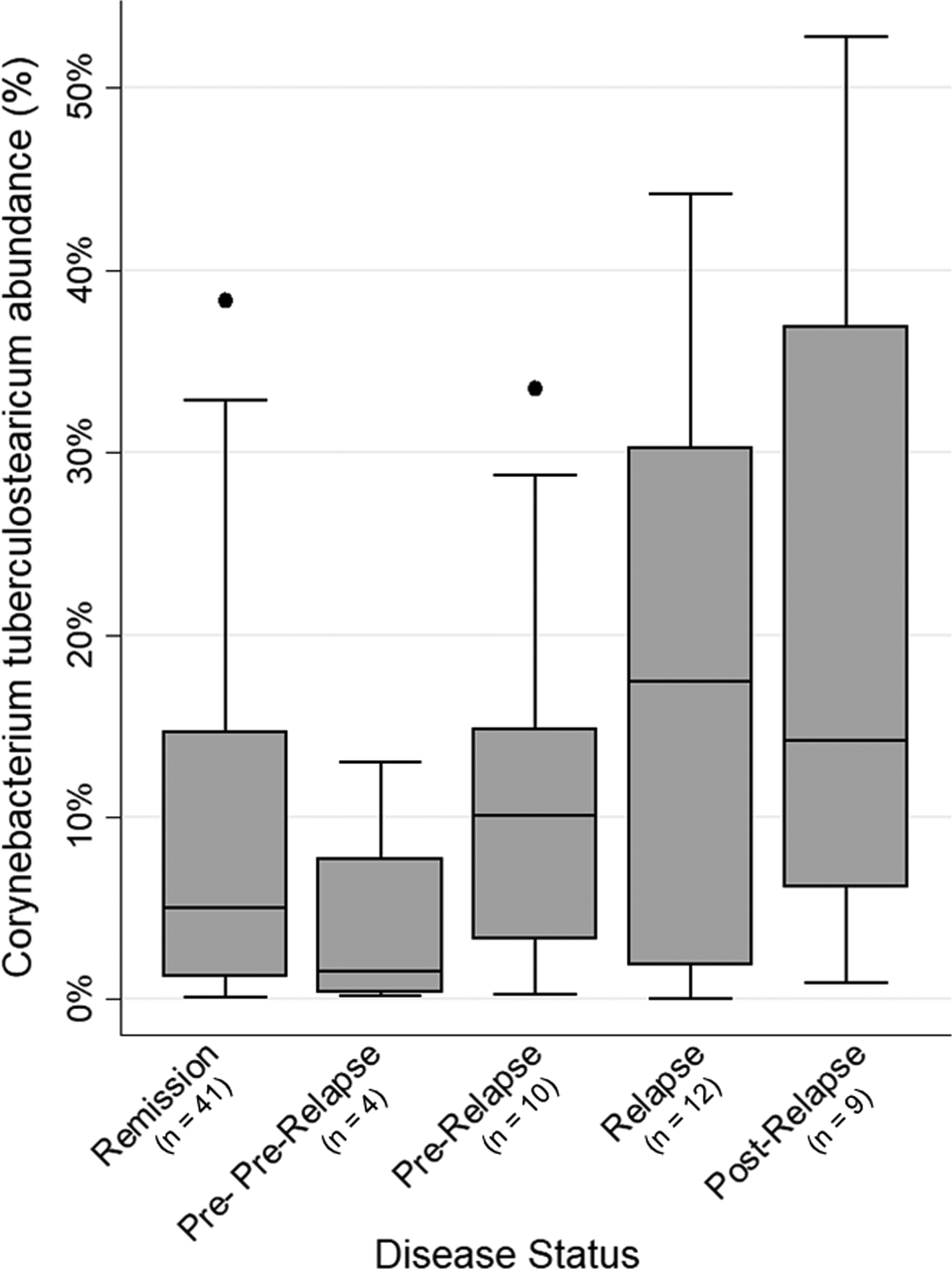
Results: Corynebacterium and Staphylococcus were the most abundant bacterial genera across all nasal samples. Patients with quiescent disease maintained a stable ratio of Corynebacterium to Staphylococcus across visits. In contrast, in patients who experienced a relapse, a significantly lower ratio was observed at the visit prior to relapse, followed by a higher ratio at the time of relapse (adjusted P < 0.01). Species-level analysis identified an association between a higher abundance of nasal Corynebacterium tuberculostearicum and 1) relapse (adjusted P = 0.04) and 2) higher PR3-ANCA levels (adjusted P = 0.02).
Conclusion: In GPA, significant changes occur in the nasal microbiome over time and are associated with disease activity. The occurrence of these changes months prior to the onset of relapse supports a pathogenic role of nasal bacteria in GPA. Our results uphold existing hypotheses implicating Staphylococcus as an instigator of disease and have generated a novel finding involving Corynebacterium as a potential mediator of disease in GPA.
© 2021, American College of Rheumatology.
Conflict of interest statement
Figures



References
-
- Hoffman GS, Kerr GS, Leavitt RY, Hallahan CW, Lebovics RS, Travis WD, et al.Wegener granulomatosis: an analysis of 158 patients. Ann Intern Med. 1992;116(6):488–98. - PubMed
-
- Pendergraft WF 3rd, Preston GA, Shah RR, Tropsha A, Carter CW Jr., Jennette JC, et al.Autoimmunity is triggered by cPR-3(105–201), a protein complementary to human autoantigen proteinase-3. Nat Med. 2004;10(1):72–9. - PubMed
-
- van Dam LS, Kraaij T, Kamerling SWA, Bakker JA, Scherer UH, Rabelink TJ, et al.Intrinsically Distinct Role of Neutrophil Extracellular Trap Formation in Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Compared to Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019;71(12):2047–58. - PMC - PubMed
-
- Tadema H, Abdulahad WH, Lepse N, Stegeman CA, Kallenberg CG, Heeringa P. Bacterial DNA motifs trigger ANCA production in ANCA-associated vasculitis in remission. Rheumatology (Oxford). 2011;50(4):689–96. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
