

Polysomnographic predictors of abnormal brainstem imaging in children
- PMID: 33682673
- PMCID: PMC8314628
- DOI: 10.5664/jcsm.9210
Polysomnographic predictors of abnormal brainstem imaging in children
Abstract
Study objectives: Evaluation of elevated central apnea-hypopnea index (CAHI) or prolonged central apneas in pediatric patients typically includes neuroimaging with a focus on brainstem pathology. There is little evidence guiding thresholds of polysomnographic variables that accurately predict abnormal neuroimaging. We sought to evaluate whether additional polysomnographic variables may help predict brainstem pathology.
Methods: A 10-year retrospective review of patients ages 1-18 years who received a brain magnetic resonance imaging (MRI) for an indication of central sleep apnea diagnosed via polysomnography was performed. Demographics, medical history, polysomnogram variables, and MRI results were compared.
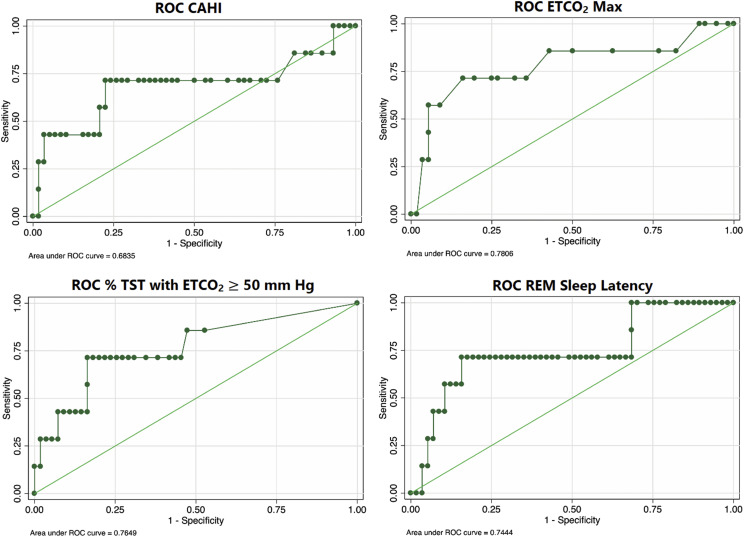
Results: This study included 65 patients (69.2% male). The median age was 5.8 years (interquartile range, 3.0-8.3). Most patients had negative (normal or nonsignificant) MRIs (n = 45, 69.2%); 20 (30.8%) had abnormal MRIs. Of the patients with abnormal MRIs, 13 (20.0%) had abnormalities unrelated to the brainstem. Seven patients (10.8%) were found to have brainstem pathology and had a median CAHI of 10.8 events/h (interquartile range, 6.5-21.9), and three of seven (42.9%) had hypoventilation and were more likely to have developmental delay, abnormal neurological examinations, and reflux. Other patients (n = 58) had a median CAHI of 5.6 events/h (interquartile range, 3.1-9.1), and seven (12.1%) had hypoventilation. Area under the curve and receiver operating characteristic curves showed a CAHI ≥ 9.5 events/h and ≥ 6.4% of total sleep time with end-tidal CO₂ ≥ 50 mm Hg predicted abnormal brainstem imaging. Prolonged central apneas did not predict abnormal brainstem imaging.
Conclusions: Most patients with central sleep apnea do not have MRIs implicating structurally abnormal brainstems. Utilizing a cutoff of CAHI of ≥ 9.5 events/h, ≥ 6.4% total sleep time with end-tidal CO₂ ≥ 50 mm Hg and/or frank hypoventilation, and additional clinical history may optimize MRI utilization in patients with central sleep apnea.
Keywords: Chiari malformation; MRI; central sleep apnea; hypoventilation; polysomnography.
© 2021 American Academy of Sleep Medicine.
Conflict of interest statement
All authors have reviewed the manuscript and have approved it in its final form. Work for this study was performed at Children’s Hospital of Philadelphia without funding from Children’s Hospital of Philadelphia or any third-party sponsors. The authors report no conflicts of interest.
Figures


References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
