

Outcomes of a clinician-directed protocol for discontinuation of complement inhibition therapy in atypical hemolytic uremic syndrome
- PMID: 33683339
- PMCID: PMC7948299
- DOI: 10.1182/bloodadvances.2020003175
Outcomes of a clinician-directed protocol for discontinuation of complement inhibition therapy in atypical hemolytic uremic syndrome
Abstract
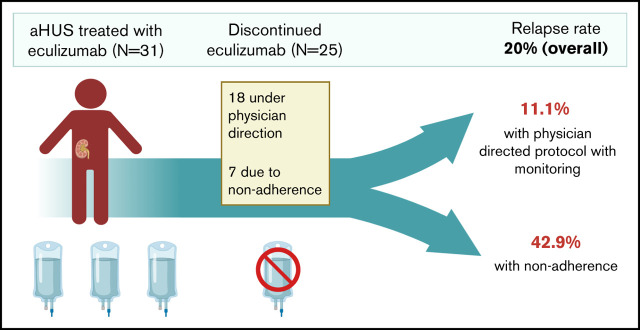
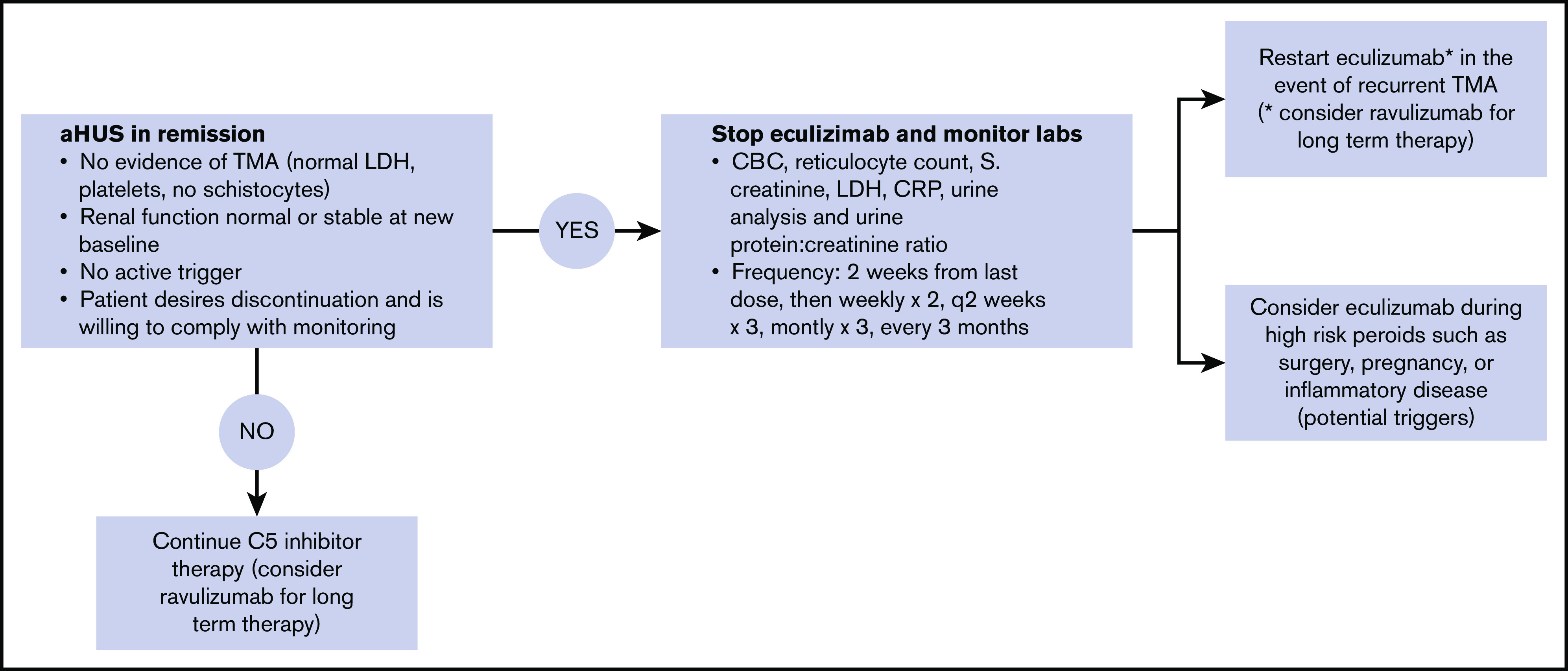
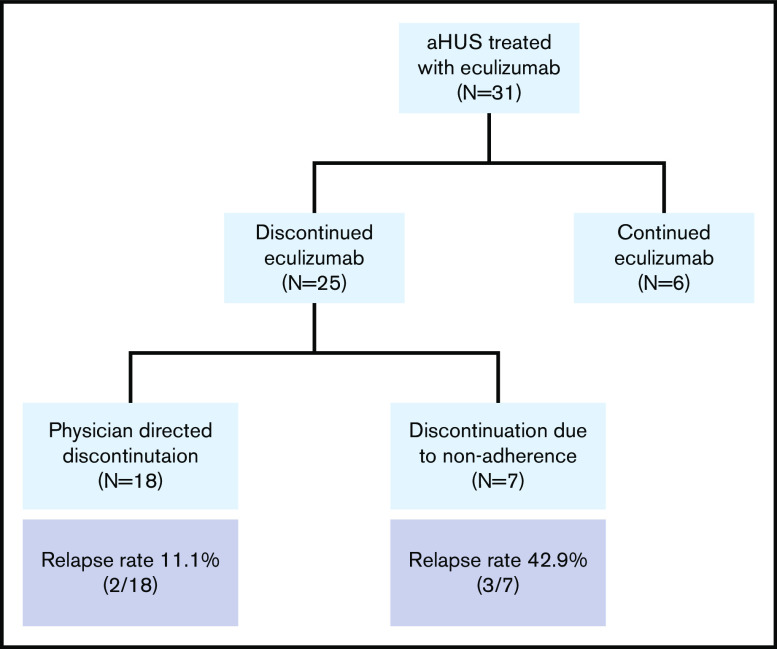
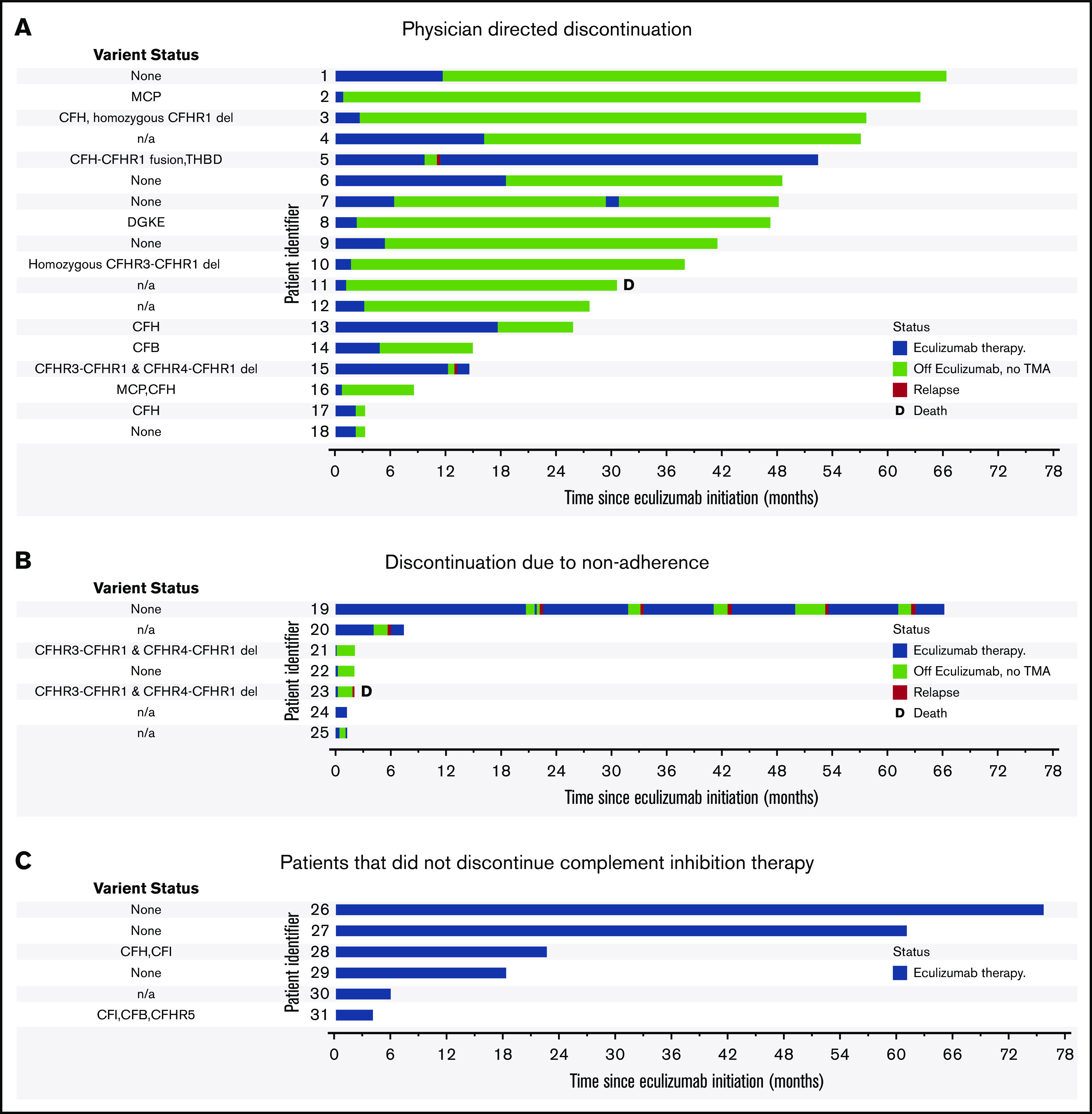
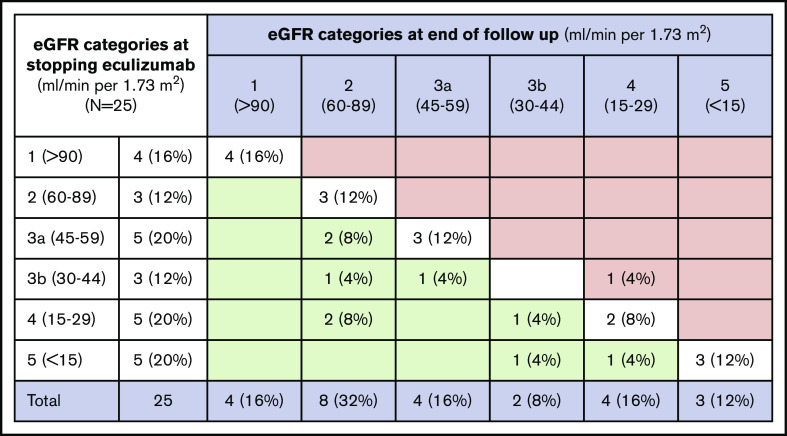
Terminal complement inhibition is the standard of care for atypical hemolytic uremic syndrome (aHUS). The optimal duration of complement inhibition is unknown, although indefinite therapy is common. Here, we present the outcomes of a physician-directed eculizumab discontinuation and monitoring protocol in a prospective cohort of 31 patients that started eculizumab for acute aHUS (and without a history of renal transplant). Twenty-five (80.6%) discontinued eculizumab therapy after a median duration on therapy of 2.37 (interquartile range: 1.06, 9.70) months. Eighteen patients discontinued per protocol and 7 because of nonadherence. Of these, 5 (20%) relapsed; however, relapse rate was higher in the case of nonadherence (42.8%) vs clinician-directed discontinuation and monitoring (11.1%). Four of 5 patients who relapsed were successfully retreated without a decline in renal function. One patient died because of recurrent aHUS and hypertensive emergency in the setting of nonadherence. Nonadherence to therapy (odds ratio, 8.25; 95% confidence interval, 1.02-66.19; P = .047) was associated with relapse, whereas the presence of complement gene variants (odds ratio, 1.39; 95% confidence interval, 0.39-4.87; P = .598) was not significantly associated with relapse. Relapse occurred in 40% (2 of 5) with a CFH or MCP variant, 33.3% (2 of 6) with other complement variants, and 0% (0 of 6) with no variants (P = .217). There was no decline in mean glomerular filtration rate from the date of stopping eculizumab until end of follow-up. In summary, eculizumab discontinuation with close monitoring is safe in most patients, with low rates of aHUS relapse and effective salvage with eculizumab retreatment in the event of recurrence.
© 2021 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Fakhouri F, Zuber J, Frémeaux-Bacchi V, Loirat C. Haemolytic uraemic syndrome. Lancet. 2017;390(10095):681-696. - PubMed
-
- Legendre CM, Licht C, Muus P, et al. . Terminal complement inhibitor eculizumab in atypical hemolytic-uremic syndrome. N Engl J Med. 2013;368(23):2169-2181. - PubMed
-
- Fakhouri F, Hourmant M, Campistol JM, et al. . Terminal complement inhibitor eculizumab in adult patients with atypical hemolytic uremic syndrome: a single-arm, open-label trial. Am J Kidney Dis. 2016;68(1):84-93. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
