

Therapeutic approaches to pediatric COVID-19: an online survey of pediatric rheumatologists
- PMID: 33683393
- PMCID: PMC7938886
- DOI: 10.1007/s00296-021-04824-4
Therapeutic approaches to pediatric COVID-19: an online survey of pediatric rheumatologists
Abstract
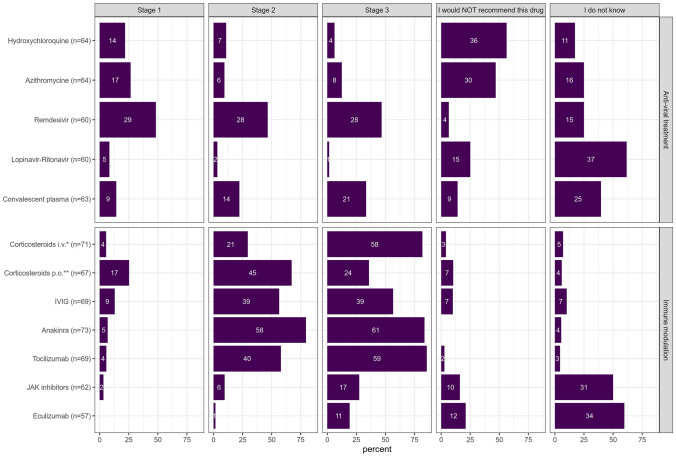
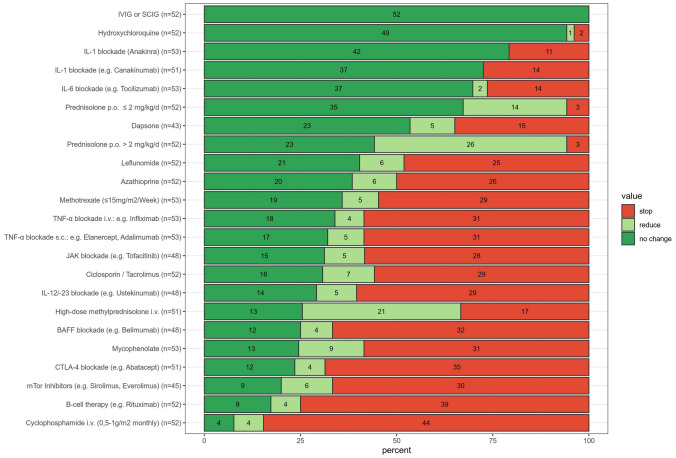
Data on therapy of COVID-19 in immunocompetent and immunosuppressed children are scarce. We aimed to explore management strategies of pediatric rheumatologists. All subscribers to international Pediatric Rheumatology Bulletin Board were invited to take part in an online survey on therapeutic approaches to COVID-19 in healthy children and children with autoimmune/inflammatory diseases (AID). Off-label therapies would be considered by 90.3% of the 93 participating respondents. In stable patients with COVID-19 on oxygen supply (stage I), use of remdesivir (48.3%), azithromycin (26.6%), oral corticosteroids (25.4%) and/or hydroxychloroquine (21.9%) would be recommended. In case of early signs of "cytokine storm" (stage II) or in critically ill patients (stage III) (a) anakinra (79.5% stage II; 83.6% stage III) or tocilizumab (58.0% and 87.0%, respectively); (b) corticosteroids (oral 67.2% stage II, intravenously 81.7% stage III); (c) intravenous immunoglobulins (both stages 56.5%); or (d) remdesivir (both stages 46.7%) were considered. In AID, > 94.2% of the respondents would not support a preventive adaptation of the immunomodulating therapy. In case of mild COVID-19, more than 50% of the respondents would continue pre-existing treatment with immunoglobulins (100%), hydroxychloroquine (94.2%), anakinra (79.2%) or canakinumab (72.5%), or tocilizumab (69.8%). Long-term corticosteroids would be reduced by 26.9% (< = 2 mg/kg/d) and 50.0% (> 2 mg/kg/day), respectively, with only 5.8% of respondents voting to discontinue the therapy. Conversely, more than 75% of respondents would refrain from administering cyclophosphamide and anti-CD20-antibodies. As evidence on management of pediatric COVID-19 is incomplete, continuous and critical expert opinion and knowledge exchange is helpful.
Keywords: Autoimmune disease; COVID-19; Children; Inflammation; Opinion poll; Pediatric rheumatology; SARS-CoV-2; Treatment.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be seen as a potential conflict of interest.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
