

Osteoid osteoma: the great mimicker
- PMID: 33683492
- PMCID: PMC7940467
- DOI: 10.1186/s13244-021-00978-8
Osteoid osteoma: the great mimicker
Abstract
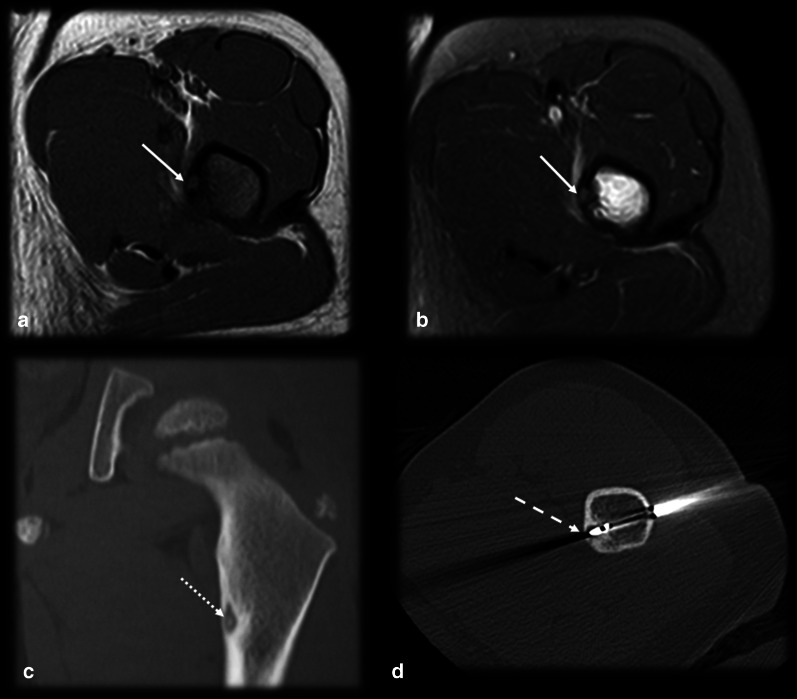
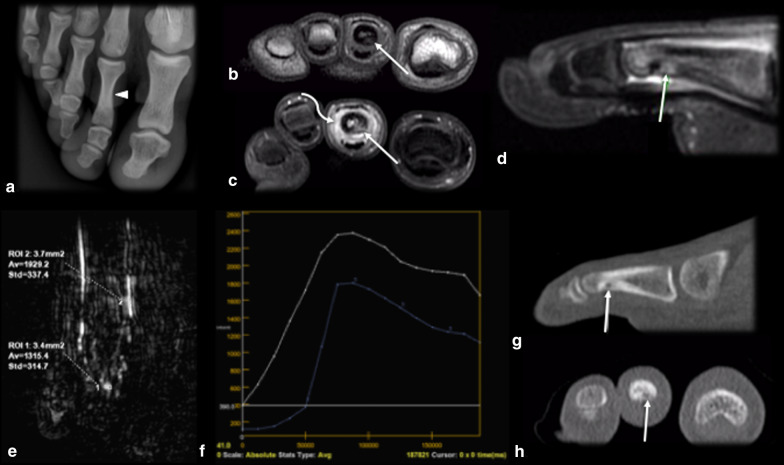
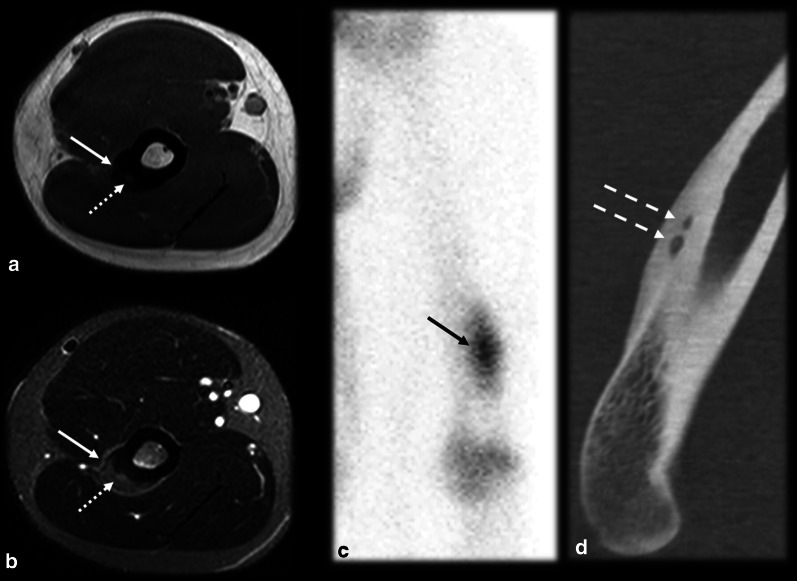
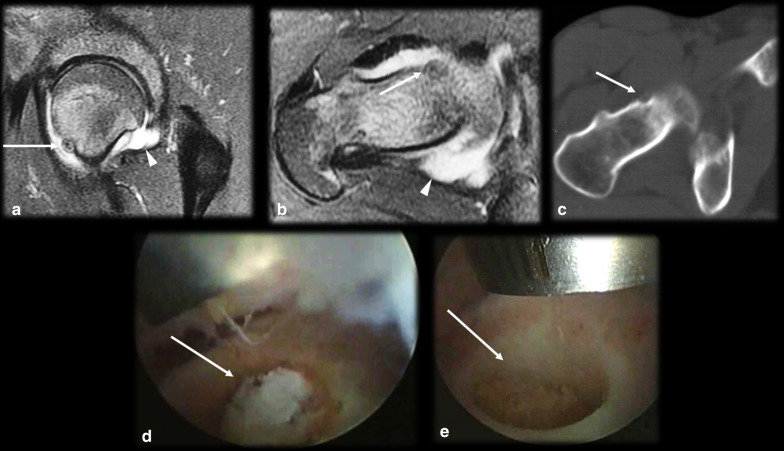
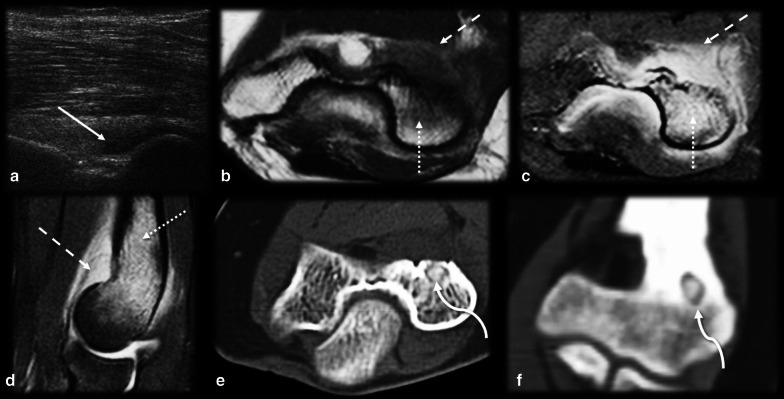
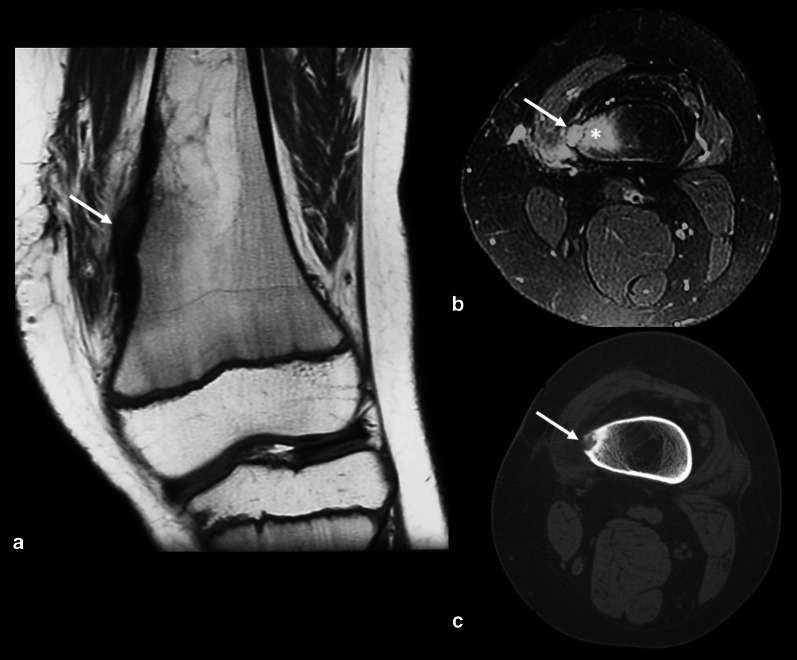
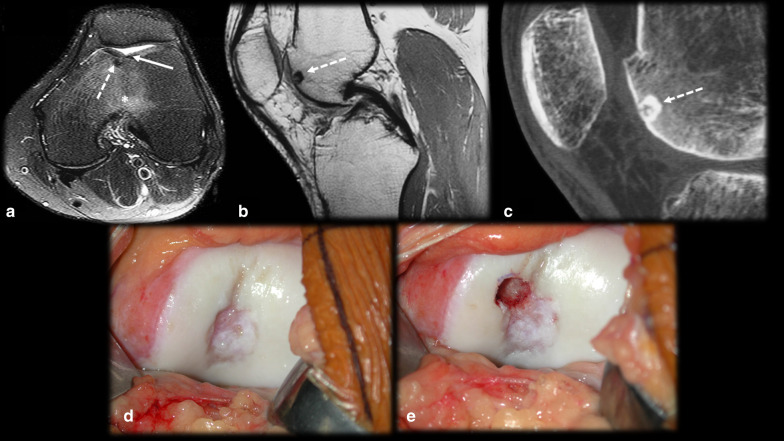
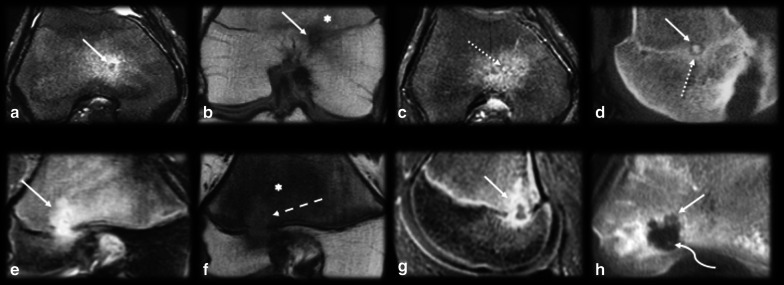
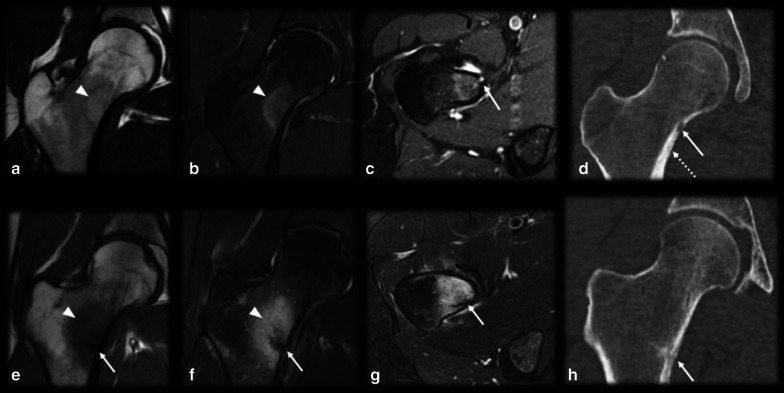
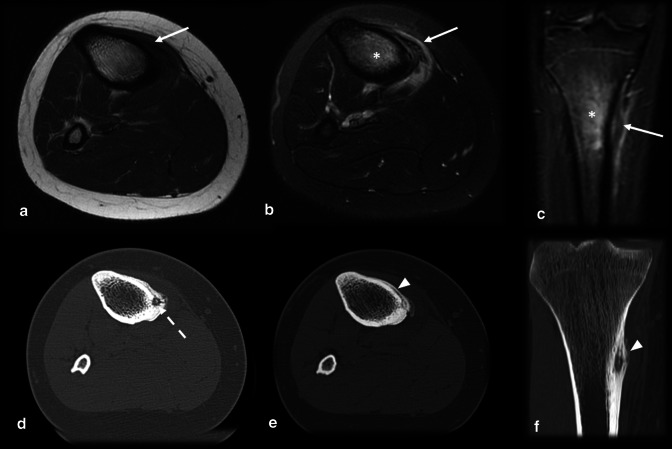
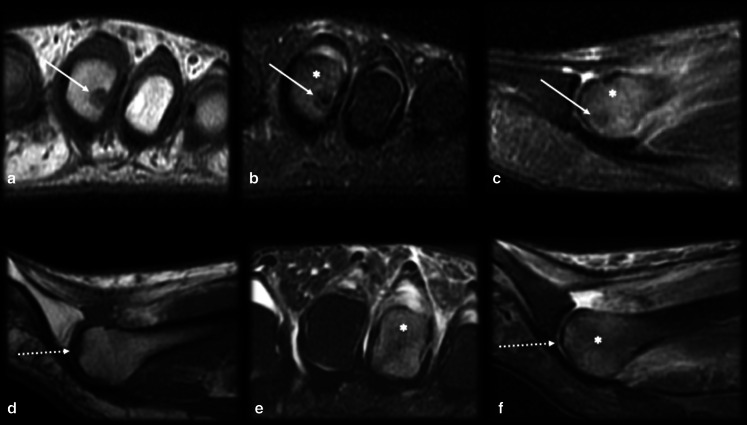
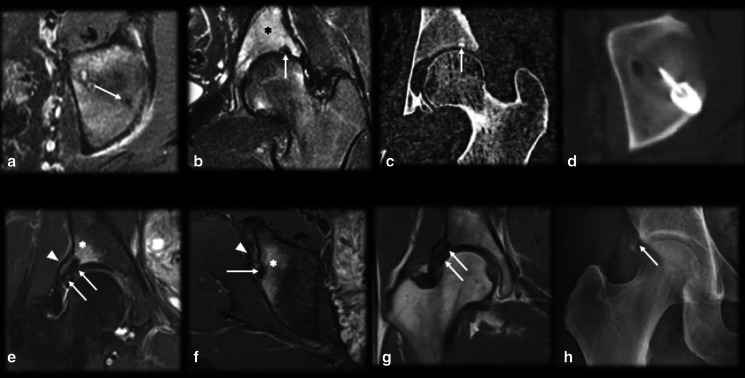
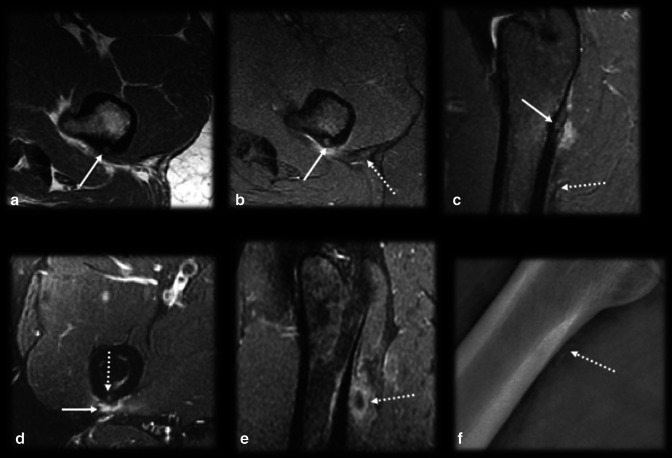
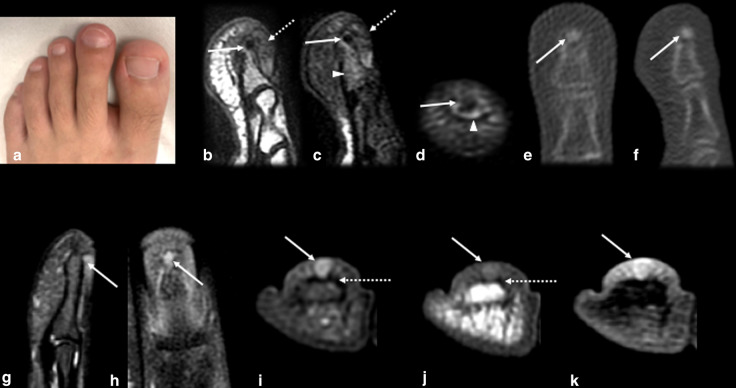
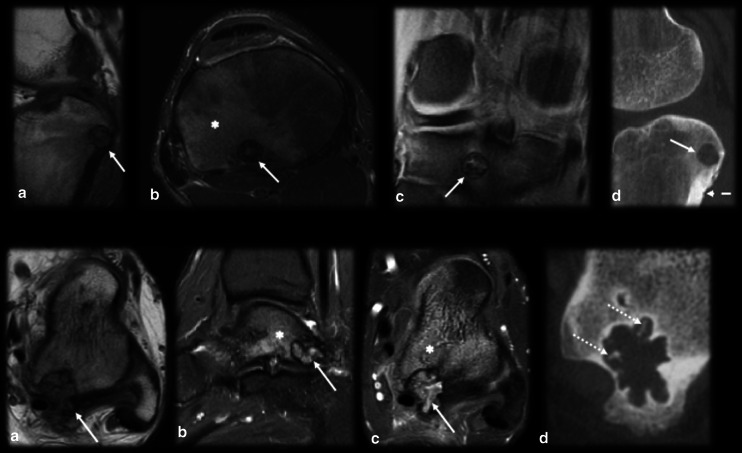
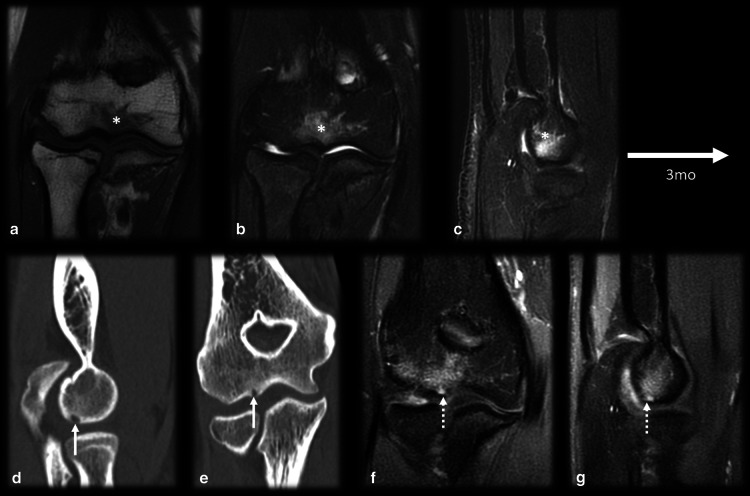
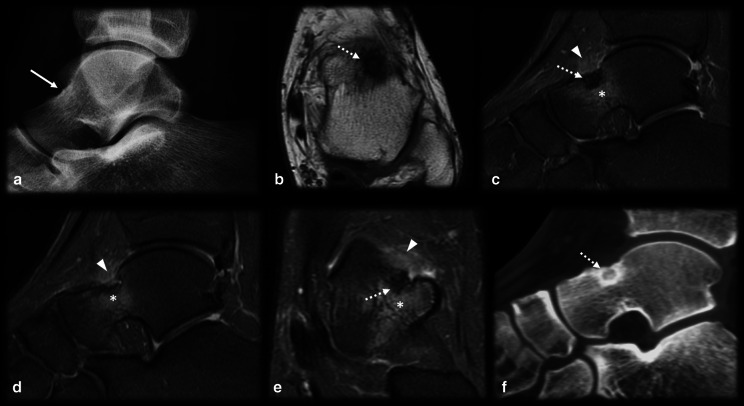
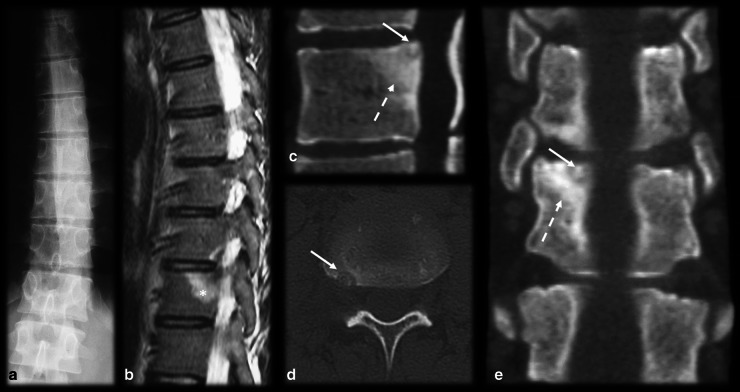
Osteoid osteoma is a painful, benign and common bone tumor that is prevalent in young adults. The typical clinical presentation consists of pain that becomes worse at night and is relieved by nonsteroidal anti-inflammatory drugs. The most common imaging finding is a lytic lesion, known as a nidus, with variable intralesional mineralization, accompanied by bone sclerosis, cortical thickening and surrounding bone marrow edema, as well as marked enhancement with intravenous contrast injection. When the lesion is located in typical locations (intracortical bone and the diaphyses of long bones), both characteristic clinical and radiological features are diagnostic. However, osteoid osteoma is a multifaceted pathology that can have unusual presentations, such as intraarticular osteoid osteoma, epiphyseal location, lesions at the extremities and multicentric nidi, and frequently present atypical clinical and radiological manifestations. In addition, many conditions may mimic osteoid osteoma and vice versa, leading to misdiagnosis. Therefore, it is essential to understand these musculoskeletal diseases and their imaging findings to increase diagnostic accuracy, enable early treatment and prevent poor prognosis.
Keywords: Bone neoplasms; Diagnosis; Differential; Magnetic resonance imaging; Osteoid; Osteoma; Tomography; X-ray computed.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Atypical Presentation of an Osteoid Osteoma With a Multicentric Nidus.Cureus. 2024 Aug 17;16(8):e67053. doi: 10.7759/cureus.67053. eCollection 2024 Aug. Cureus. 2024. PMID: 39286680 Free PMC article.
-
Osteoid osteoma of the rib masquerading as pain due to trauma: Removed by rib resection using preoperative CT-scan guidance.Int J Surg Case Rep. 2023 Feb;103:107877. doi: 10.1016/j.ijscr.2023.107877. Epub 2023 Jan 9. Int J Surg Case Rep. 2023. PMID: 36706671 Free PMC article.
-
Osteoid Osteoma, a Diagnostic Problem: A Series of Atypical and Mimicking Presentations and Review of the Recent Literature.J Clin Med. 2023 Apr 5;12(7):2721. doi: 10.3390/jcm12072721. J Clin Med. 2023. PMID: 37048803 Free PMC article. Review.
-
Radiologic diagnosis of osteoid osteoma: from simple to challenging findings.Radiographics. 2010 May;30(3):737-49. doi: 10.1148/rg.303095120. Radiographics. 2010. PMID: 20462991
-
Osteoid osteoma and osteoblastoma.J Am Acad Orthop Surg. 2011 Nov;19(11):678-89. doi: 10.5435/00124635-201111000-00004. J Am Acad Orthop Surg. 2011. PMID: 22052644 Review.
Cited by
-
Current Approaches to Osteoid Osteoma and Minimally Invasive Surgery-A Minireview and a Case Report.J Clin Med. 2022 Sep 30;11(19):5806. doi: 10.3390/jcm11195806. J Clin Med. 2022. PMID: 36233673 Free PMC article.
-
Imaging mimickers of MSK infection.Skeletal Radiol. 2024 Oct;53(10):2227-2246. doi: 10.1007/s00256-024-04763-8. Epub 2024 Aug 16. Skeletal Radiol. 2024. PMID: 39150526 Review.
-
A Reminder for Chronic Ankle Pain: Case Report of Talar Osteoid Osteoma with Late Diagnosis.J Orthop Case Rep. 2022 Aug;12(8):42-46. doi: 10.13107/jocr.2022.v12.i08.2958. J Orthop Case Rep. 2022. PMID: 36687487 Free PMC article.
-
Accuracy of clinical diagnosis, imaging methods, and biopsy in tumours and pseudo-tumours of the hand.Quant Imaging Med Surg. 2024 Nov 1;14(11):7803-7816. doi: 10.21037/qims-24-347. Epub 2024 Oct 23. Quant Imaging Med Surg. 2024. PMID: 39544478 Free PMC article.
-
Osteoid osteoma of the rib: A report of an extremely rare condition.Int J Surg Case Rep. 2022 May;94:107139. doi: 10.1016/j.ijscr.2022.107139. Epub 2022 May 6. Int J Surg Case Rep. 2022. PMID: 35658306 Free PMC article.
References
-
- Jaffe HL. "Osteoid-osteoma": a benign osteoblastic tumor composed of osteoid and atypical bone. Arch Surg. 1935;31(5):709–728. doi: 10.1001/archsurg.1935.01180170034003. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
