

Rubber band ligation versus haemorrhoidectomy for the treatment of grade II-III haemorrhoids: a systematic review and meta-analysis of randomised controlled trials
- PMID: 33683503
- PMCID: PMC8124052
- DOI: 10.1007/s10151-021-02430-x
Rubber band ligation versus haemorrhoidectomy for the treatment of grade II-III haemorrhoids: a systematic review and meta-analysis of randomised controlled trials
Abstract
Background: The aim of this study was to review clinical outcome of haemorrhoidectomy and rubber band ligation in grade II-III haemorrhoids.
Methods: A systematic review was conducted. Medline, Embase, Cochrane Library, Clinicaltrials.gov, and the WHO International Trial Registry Platform were searched, from inception until May 2018, to identify randomised clinical trials comparing rubber band ligation with haemorrhoidectomy for grade II-III haemorrhoids. The primary outcome was control of symptoms. Secondary outcomes included postoperative pain, postoperative complications, anal continence, patient satisfaction, quality of life and healthcare costs were assessed. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed.
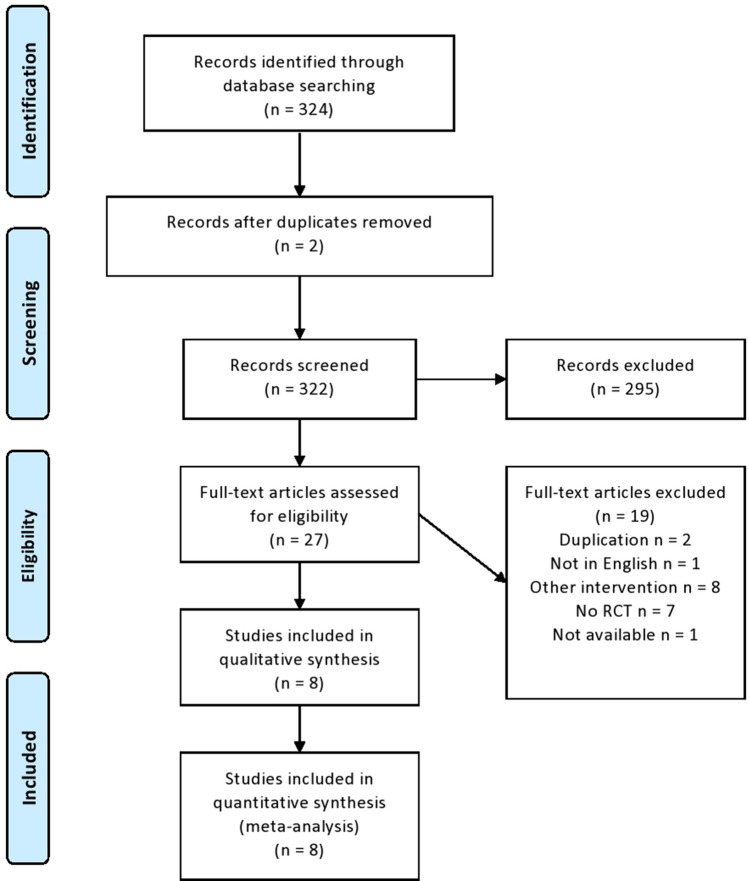
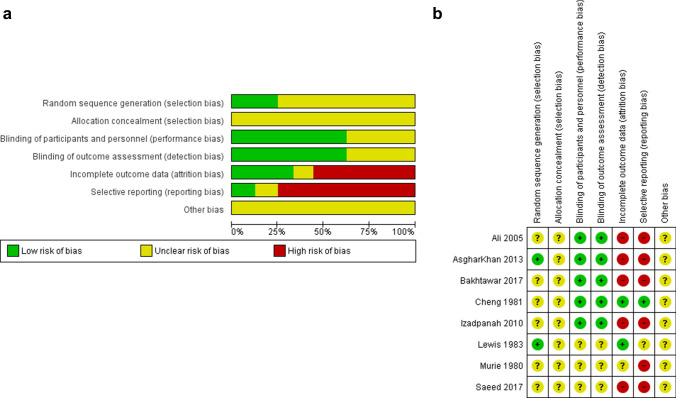
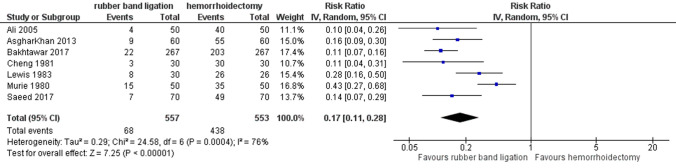
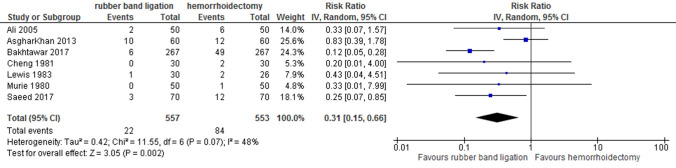
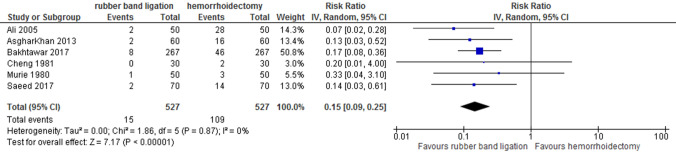
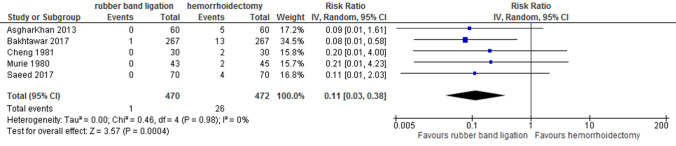
Results: Three hundred and twenty-four studies were identified. Eight trials met the inclusion criteria. All trials were of moderate methodological quality. Outcome measures were diverse and not clearly defined. Control of symptoms was better following haemorrhoidectomy. Patients had less pain after rubber band ligation. There were more complications (bleeding, urinary retention, anal incontinence/stenosis) in the haemorrhoidectomy group. Patient satisfaction was equal in both groups. There were no data on quality of life and healthcare costs except that in one study patients resumed work more early after rubber band ligation.
Conclusions: Haemorrhoidectomy seems to provide better symptom control but at the cost of more pain and complications. However, due to the poor quality of the studies analysed/it is not possible to determine which of the two procedures provides the best treatment for grade II-III haemorrhoids. Further studies focusing on clearly defined outcome measurements taking patients perspective and economic impact into consideration are required.
Keywords: Complications; Haemorrhoidectomy; Haemorrhoids; Reintervention; Rubber band ligation.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- NIVEL, ‘Incidence and prevalence rates of Haemorrhoids in Dutch general practice classified by sex in 2017 (per 1000 patient years)’. Retrieved October 2020 [Online]. Available: https://www.nivel.nl/nl/nivel-zorgregistraties-eerste-lijn/jaarcijfers-a....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
