

Emergency room comprehensive assessment of demographic, radiological, laboratory and clinical data of patients with COVID-19: determination of its prognostic value for in-hospital mortality
- PMID: 33683539
- PMCID: PMC7938271
- DOI: 10.1007/s11739-021-02669-0
Emergency room comprehensive assessment of demographic, radiological, laboratory and clinical data of patients with COVID-19: determination of its prognostic value for in-hospital mortality
Abstract
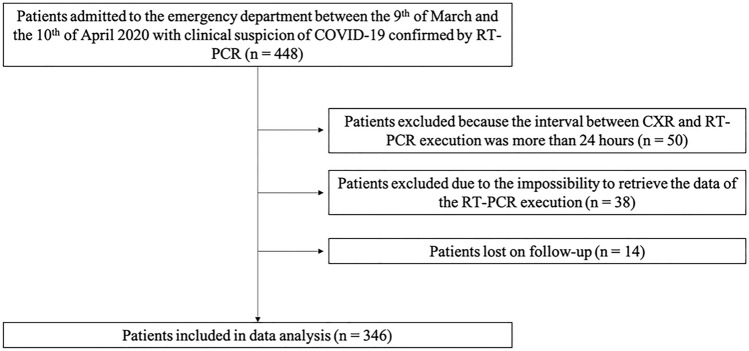
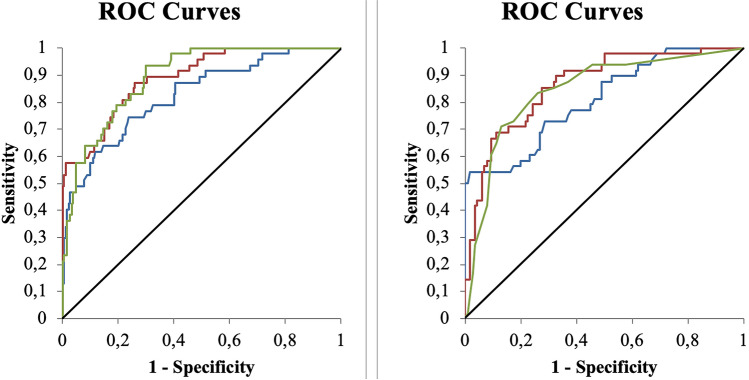
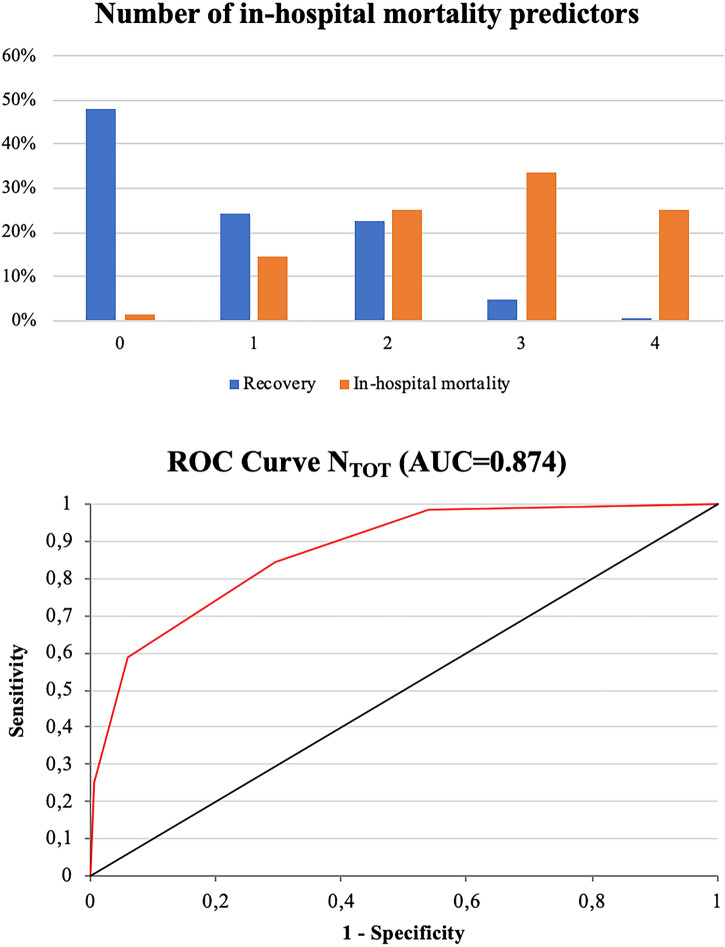
Mortality risk in COVID-19 patients is determined by several factors. The aim of our study was to adopt an integrated approach based on clinical, laboratory and chest x-ray (CXR) findings collected at the patient's admission to Emergency Room (ER) to identify prognostic factors. Retrospective study on 346 consecutive patients admitted to the ER of two North-Western Italy hospitals between March 9 and April 10, 2020 with clinical suspicion of COVID-19 confirmed by reverse transcriptase-polymerase reaction chain test (RT-PCR), CXR performed within 24 h (analyzed with two different scores) and recorded prognosis. Clinical and laboratory data were collected. Statistical analysis on the features of 83 in-hospital dead vs 263 recovered patients was performed with univariate (uBLR), multivariate binary logistic regression (mBLR) and ROC curve analysis. uBLR identified significant differences for several variables, most of them intertwined by multiple correlations. mBLR recognized as significant independent predictors for in-hospital mortality age > 75 years, C-reactive protein (CRP) > 60 mg/L, PaO2/FiO2 ratio (P/F) < 250 and CXR "Brixia score" > 7. Among the patients with at least two predictors, the in-hospital mortality rate was 58% against 6% for others [p < 0.0001; RR = 7.6 (4.4-13)]. Patients over 75 years had three other predictors in 35% cases against 10% for others [p < 0.0001, RR = 3.5 (1.9-6.4)]. The greatest risk of death from COVID-19 was age above 75 years, worsened by elevated CRP and CXR score and reduced P/F. Prompt determination of these data at admission to the emergency department could improve COVID-19 pretreatment risk stratification.
Keywords: Chest X-ray; Coronavirus disease 2019 (COVID-19); Outcome; Prognosis; Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
© 2021. The Author(s).
Conflict of interest statement
Authors declare no conflict of interests for this article.
Figures

References
-
- Coronavirus. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accessed 23 Nov 2020
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
