

Differentiating uterine sarcoma from leiomyoma: BET1T2ER Check!
- PMID: 33684303
- PMCID: PMC9327746
- DOI: 10.1259/bjr.20201332
Differentiating uterine sarcoma from leiomyoma: BET1T2ER Check!
Abstract
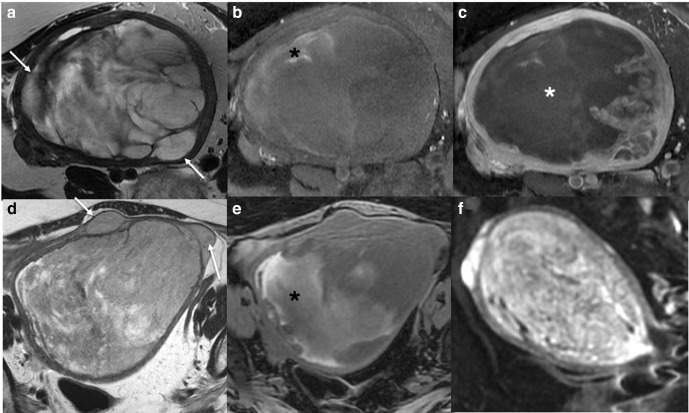
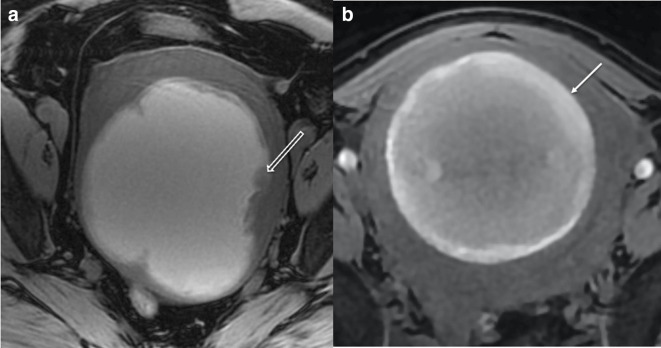
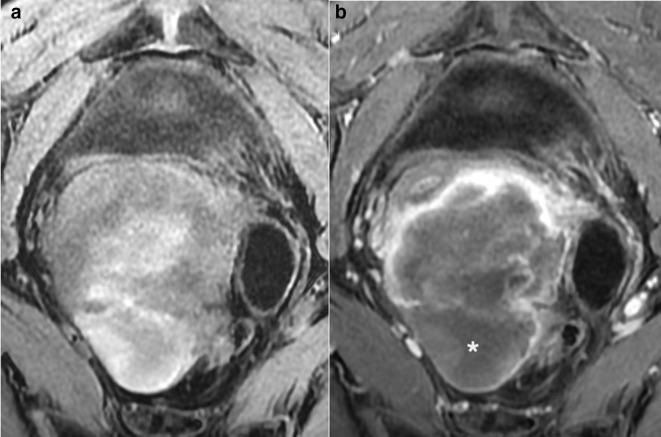
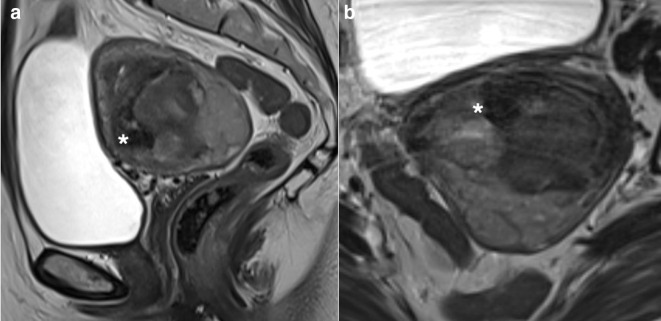
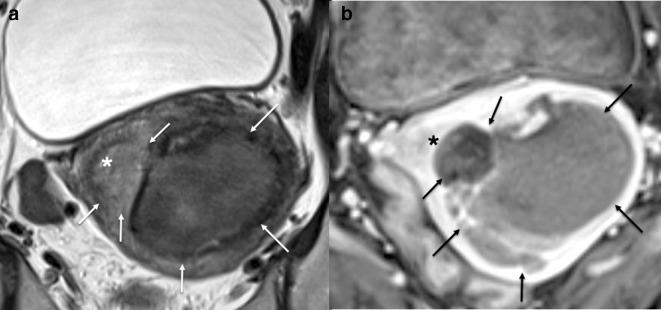
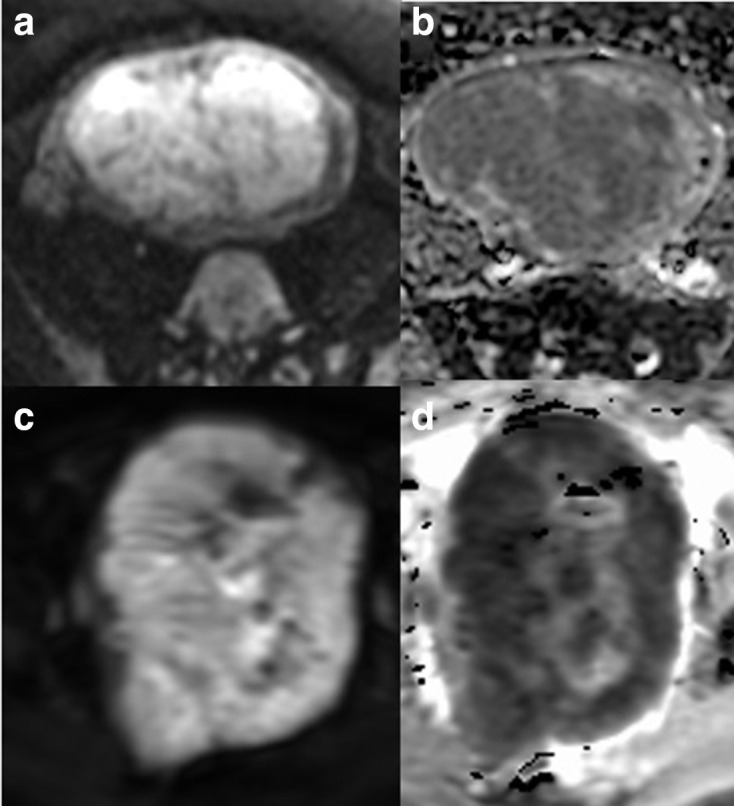
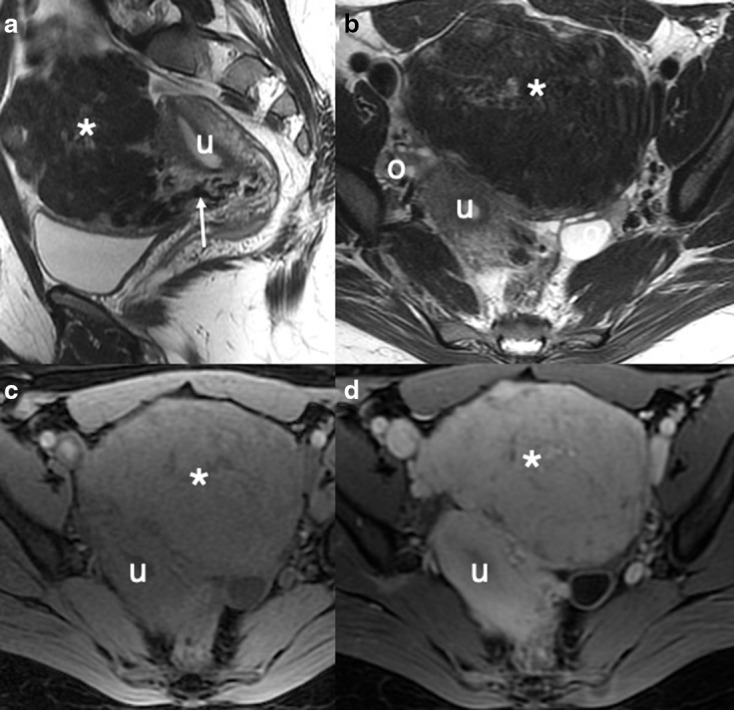
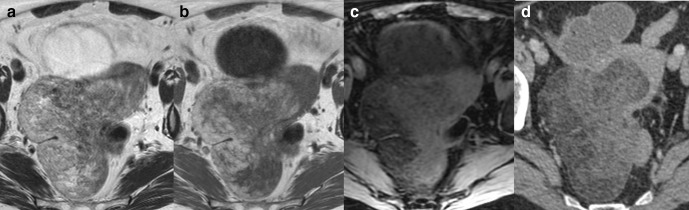
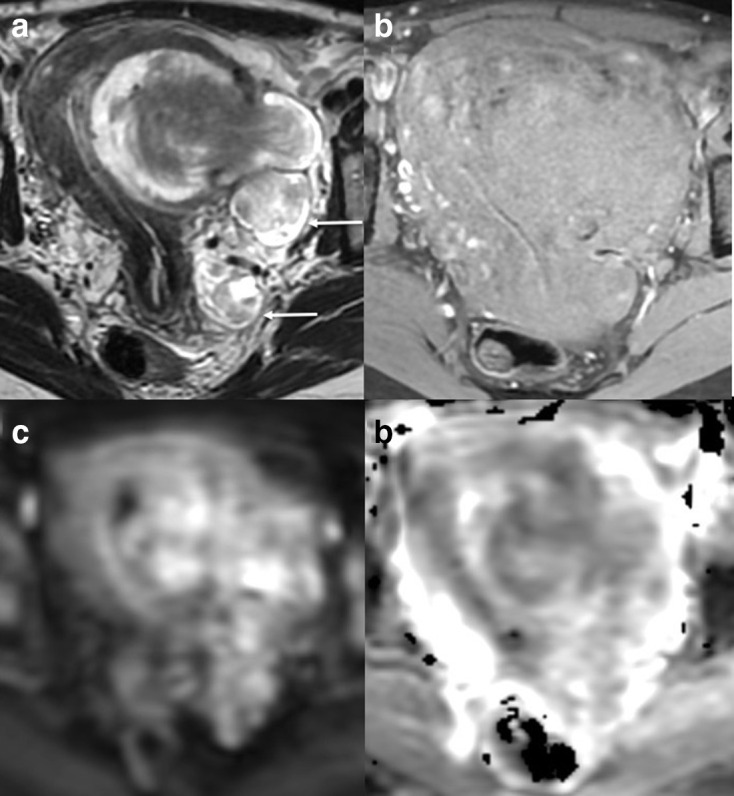
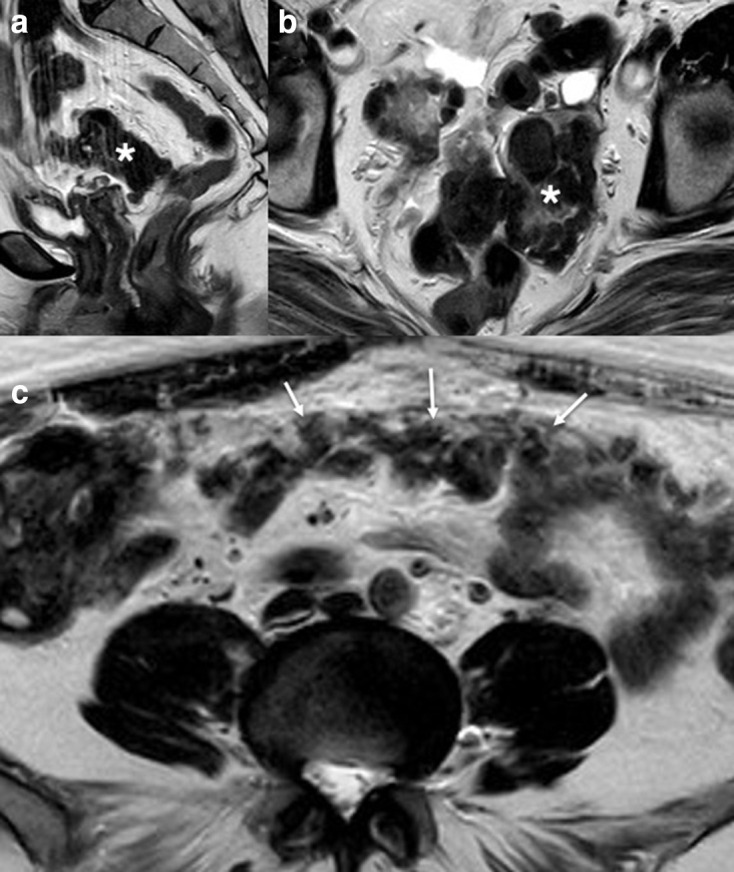
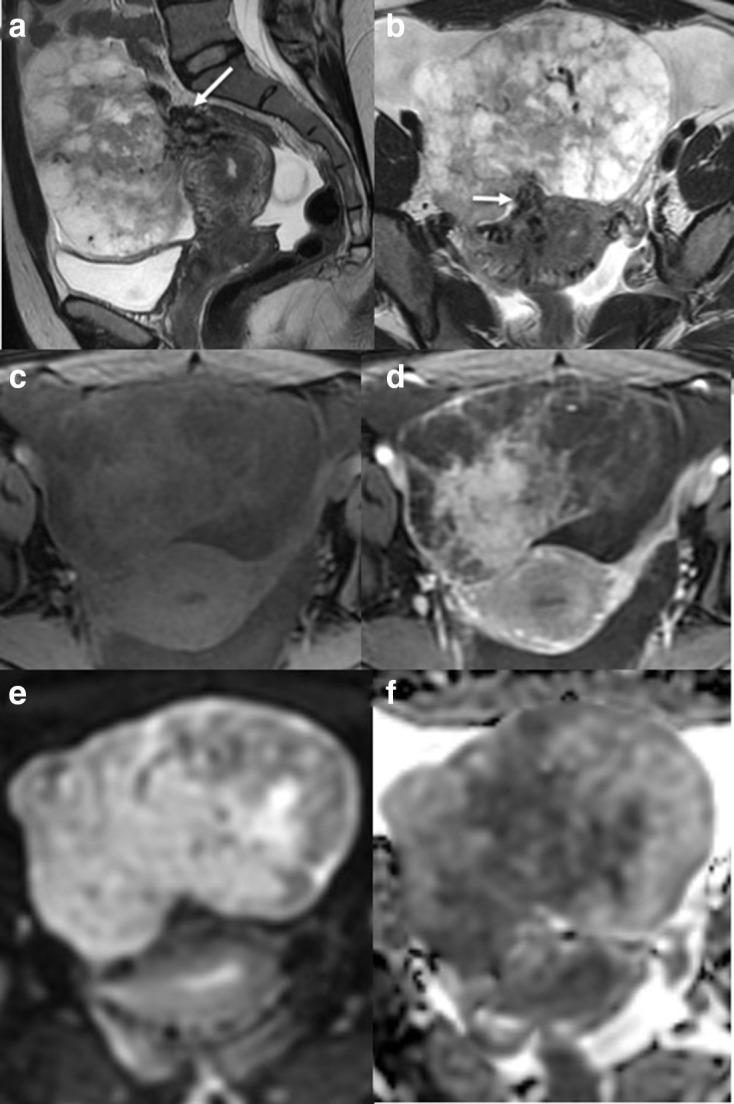
Although rare, uterine sarcoma is a diagnosis that no one wants to miss. Often benign leiomyomas (fibroids) and uterine sarcomas can be differentiated due to the typical low T2 signal intensity contents and well-defined appearances of benign leiomyomas compared to the suspicious appearances of sarcomas presenting as large uterine masses with irregular outlines and intermediate T2 signal intensity together with possible features of secondary spread. The problem is when these benign lesions are atypical causing suspicious imaging features. This article provides a review of the current literature on imaging features of atypical fibroids and uterine sarcomas with an aide-memoire BET1T2ER Check! to help identify key features more suggestive of a uterine sarcoma.
Figures

References
-
- Lakhman Y, Veeraraghavan H, Chaim J, Feier D, Goldman DA, Moskowitz CS, et al. Differentiation of uterine leiomyosarcoma from atypical leiomyoma: diagnostic accuracy of qualitative MR imaging features and feasibility of texture analysis. Eur Radiol 2017; 27: 2903–15. doi: 10.1007/s00330-016-4623-9 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
