

Diagnostic and procedural intraoperative ultrasound: technique, tips and tricks for optimizing results
- PMID: 33684305
- PMCID: PMC8506184
- DOI: 10.1259/bjr.20201406
Diagnostic and procedural intraoperative ultrasound: technique, tips and tricks for optimizing results
Abstract
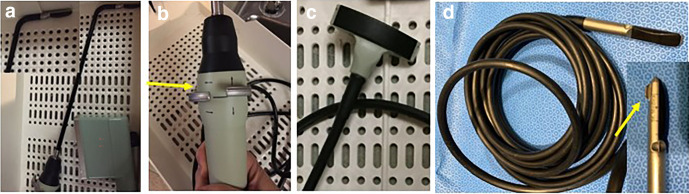
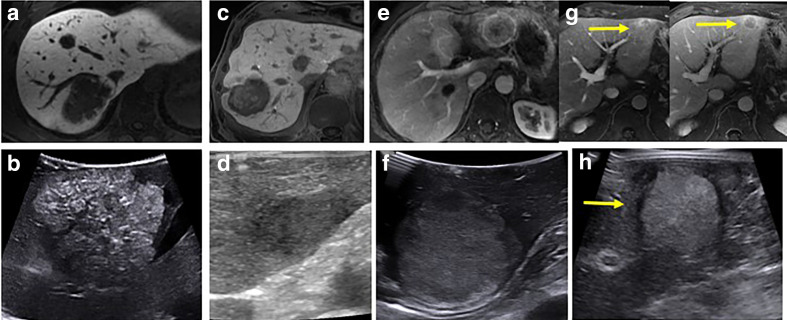
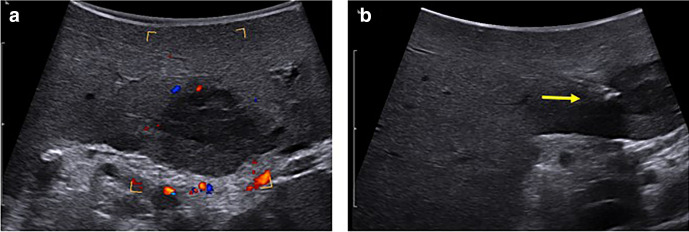
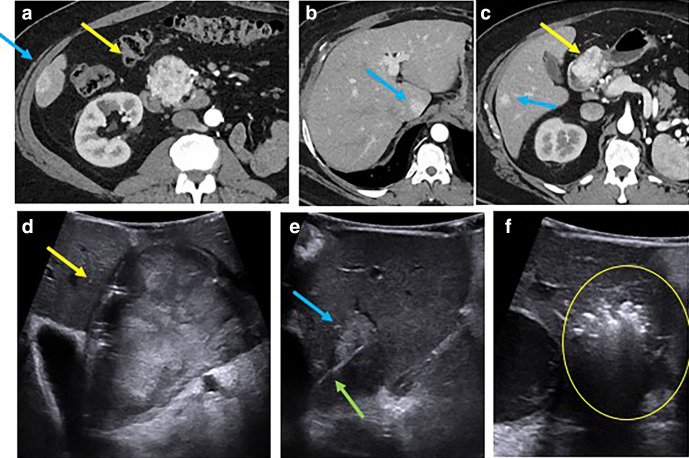
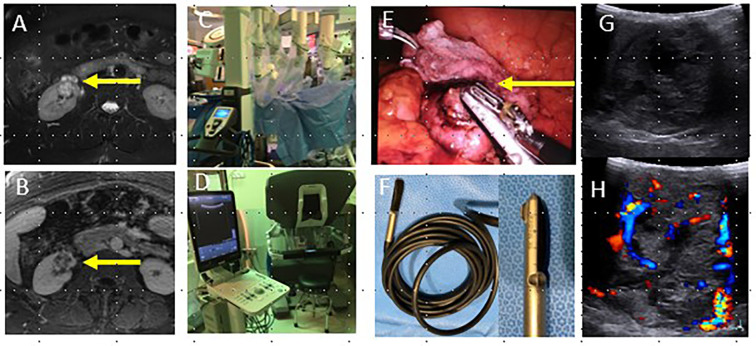
Intraoperative ultrasound (IOUS) is a valuable adjunctive tool that can provide real-time diagnostic information in surgery that has the potential to alter patient management and decrease complications. Lesion localization, characterization and staging can be performed, as well as surveying for additional lesions and metastatic disease. IOUS is commonly used in the liver for hepatic metastatic disease and hepatocellular carcinoma, in the pancreas for neuroendocrine tumors, and in the kidney for renal cell carcinoma. IOUS allows real-time evaluation of vascular patency and perfusion in organ transplantation and allows for early intervention for anastomotic complications. It can also be used to guide intraoperative procedures such as biopsy, fiducial placement, radiation, or ablation. A variety of adjuncts including microbubble contrast and elastography may provide additional information at IOUS. It is important for the radiologist to be familiar with the available equipment, common clinical indications, technique, relevant anatomy and intraoperative imaging appearance to optimize performance of this valuable imaging modality.
Figures
Similar articles
-
Value of contrast-enhanced intraoperative ultrasound for cirrhotic patients with hepatocellular carcinoma: a report of 20 cases.World J Gastroenterol. 2008 Jul 7;14(25):4005-10. doi: 10.3748/wjg.14.4005. World J Gastroenterol. 2008. PMID: 18609684 Free PMC article.
-
Contrast-enhanced ultrasound: Improving the preoperative staging of hepatocellular carcinoma and guiding individual treatment.World J Gastroenterol. 2014 Sep 21;20(35):12628-36. doi: 10.3748/wjg.v20.i35.12628. World J Gastroenterol. 2014. PMID: 25253968 Free PMC article.
-
Intraoperative high resolution linear contrast enhanced ultrasound (IOUS) for detection of microvascularization of malignant liver lesions before surgery or radiofrequeny ablation.Clin Hemorheol Microcirc. 2012;50(1-2):65-77. doi: 10.3233/CH-2011-1444. Clin Hemorheol Microcirc. 2012. PMID: 22538536
-
State of the art of intraoperative ultrasound in liver surgery: current use for staging and resection guidance.Ultraschall Med. 2014 Dec;35(6):500-11; quiz 512-3. doi: 10.1055/s-0034-1385515. Epub 2014 Dec 4. Ultraschall Med. 2014. PMID: 25474100 Review.
-
Intraoperative ultrasonography in liver cancer.Surg Oncol Clin N Am. 2003 Jan;12(1):91-103. doi: 10.1016/s1055-3207(02)00084-4. Surg Oncol Clin N Am. 2003. PMID: 12735132 Review.
Cited by
-
Multicenter Study on the Clinical Characteristics, Diagnosis, and Treatment Outcomes of Insulinoma: Insights From 15 Medical Centres.Clin Endocrinol (Oxf). 2025 Jul;103(1):57-65. doi: 10.1111/cen.15255. Epub 2025 Apr 25. Clin Endocrinol (Oxf). 2025. PMID: 40275816 Free PMC article.
-
Diagnostic and therapeutic understanding of multiple foci hepatic epithelioid haemangioendothelioma: A case report.Oncol Lett. 2025 Jun 3;30(2):383. doi: 10.3892/ol.2025.15129. eCollection 2025 Aug. Oncol Lett. 2025. PMID: 40535097 Free PMC article.
-
Enhancing Surgical Guidance: Deep Learning-Based Liver Vessel Segmentation in Real-Time Ultrasound Video Frames.Cancers (Basel). 2024 Oct 30;16(21):3674. doi: 10.3390/cancers16213674. Cancers (Basel). 2024. PMID: 39518111 Free PMC article.
-
Diagnostic Accuracy of Sonazoid-Enhanced Ultrasonography for Detection of Liver Metastasis.Med Sci (Basel). 2025 Apr 9;13(2):42. doi: 10.3390/medsci13020042. Med Sci (Basel). 2025. PMID: 40265389 Free PMC article.
-
Non-contrast ultrasound image analysis for spatial and temporal distribution of blood flow after spinal cord injury.Sci Rep. 2024 Jan 6;14(1):714. doi: 10.1038/s41598-024-51281-7. Sci Rep. 2024. PMID: 38184676 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
