

Atraumatic fractures of the femur
- PMID: 33684312
- PMCID: PMC8506166
- DOI: 10.1259/bjr.20201457
Atraumatic fractures of the femur
Abstract
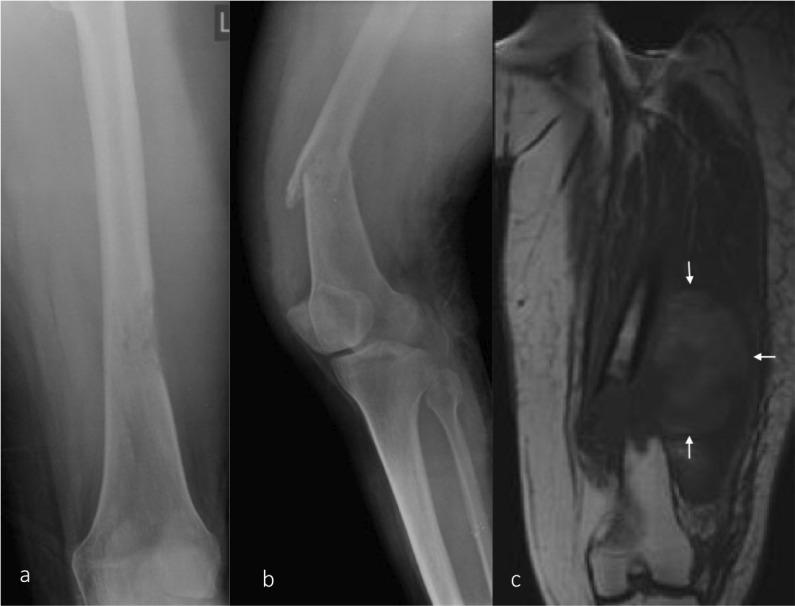
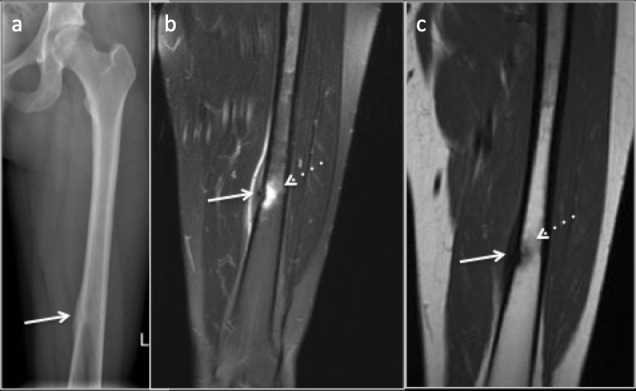
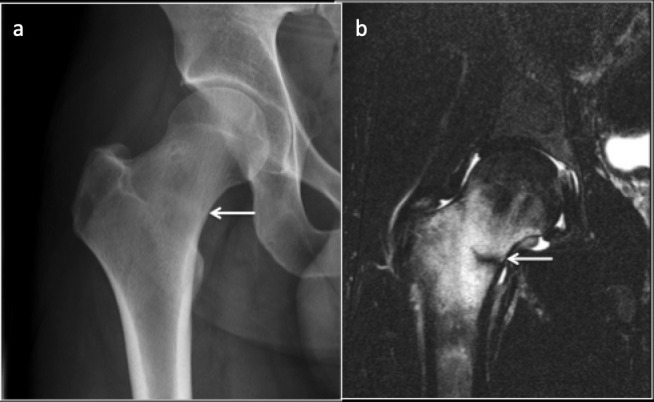
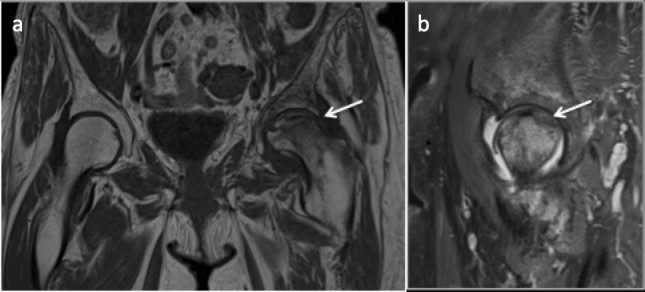
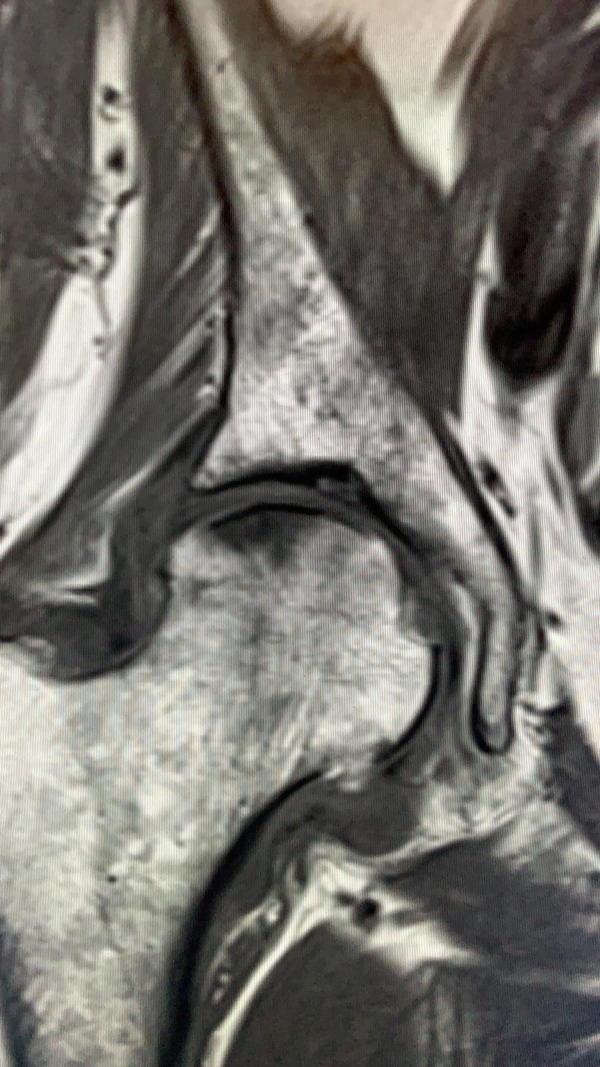
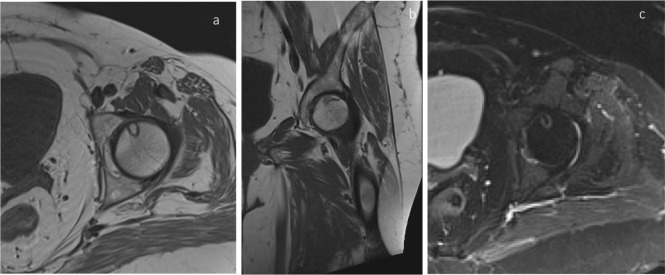
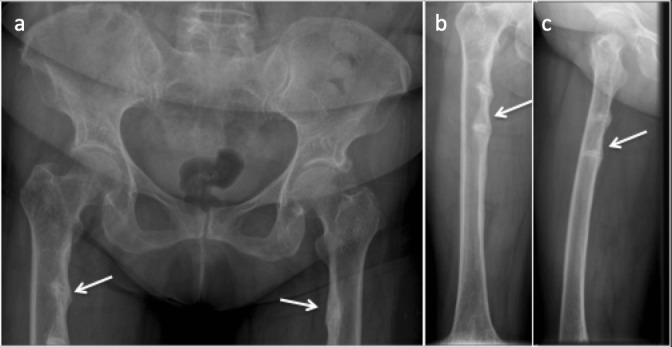
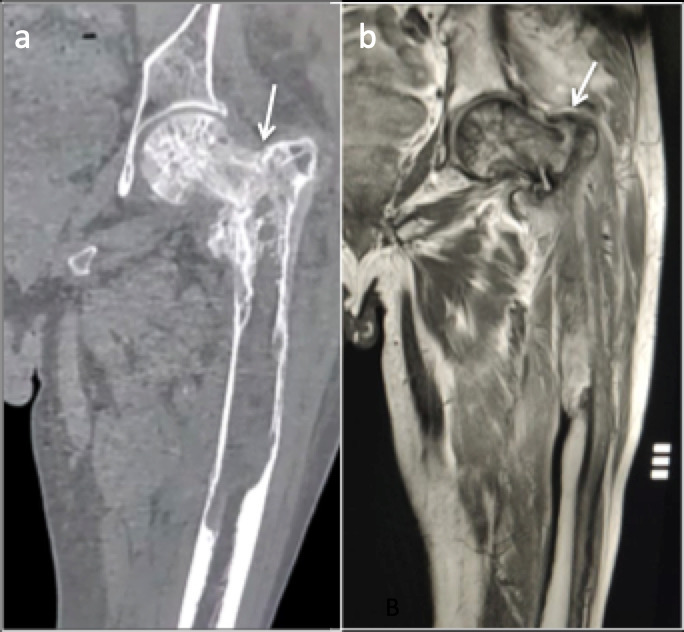
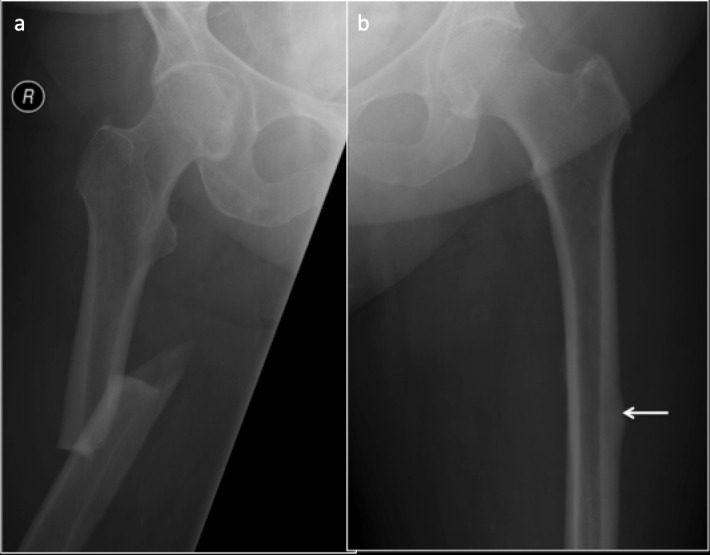
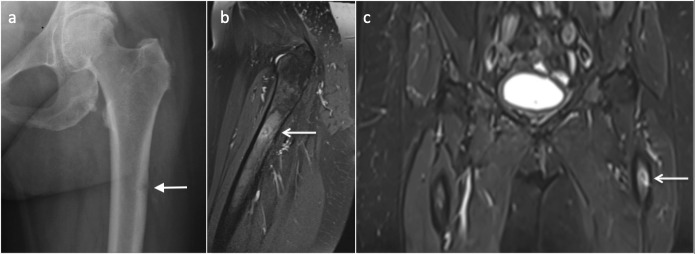
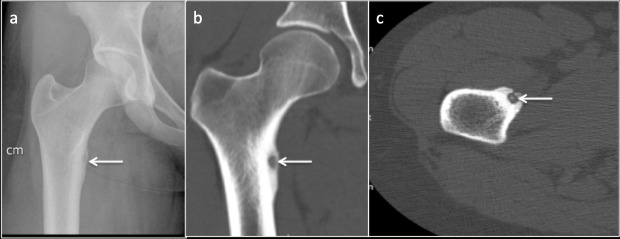
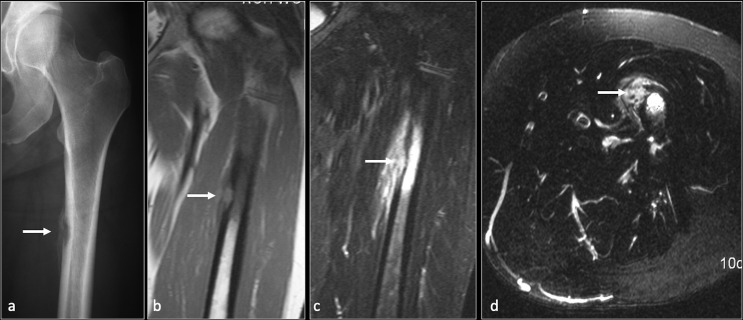
Atraumatic fractures of femur, although not as common as traumatic fractures, are frequently encountered in the clinical practice. They present with non-specific symptoms and can be occult on initial imaging making their diagnosis difficult, sometimes resulting in complications. Overlapping terminologies used to describe these fractures may hamper effective communication between the radiologist and the clinician. In this article, we review various atraumatic fractures of femur, terminologies used to describe them, their imaging findings and differential diagnosis. The article also describes the aetiology, pathophysiology and relevant biomechanics behind these fractures. An approach to atraumatic femoral fractures has been outlined.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
