

Fecal Mycobiota Combined With Host Immune Factors Distinguish Clostridioides difficile Infection From Asymptomatic Carriage
- PMID: 33684427
- PMCID: PMC8169571
- DOI: 10.1053/j.gastro.2021.02.069
Fecal Mycobiota Combined With Host Immune Factors Distinguish Clostridioides difficile Infection From Asymptomatic Carriage
Abstract
Background & aims: Although the role of gut microbiota in Clostridioides difficile infection (CDI) has been well established, little is known about the role of mycobiota in CDI. Here, we performed mycobiome data analysis in a well-characterized human cohort to evaluate the potential of using gut mycobiota features for CDI diagnosis.
Methods: Stool samples were collected from 118 hospital patients, divided into 3 groups: CDI (n = 58), asymptomatic carriers (Carrier, n = 28), and Control (n = 32). The nuclear ribosomal DNA internal transcribed spacer 2 was sequenced using the Illumina HiSeq platform to assess the fungal composition. Downstream statistical analyses (including Alpha diversity analysis, ordination analysis, differential abundance analysis, fungal correlation network analysis, and classification analysis) were then performed.
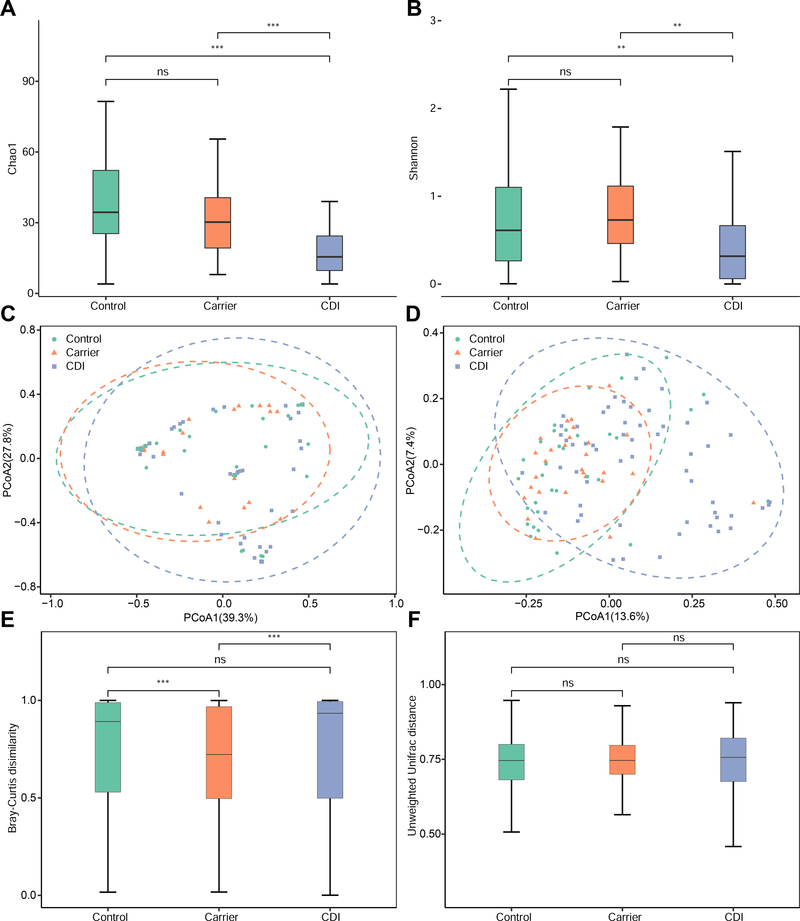
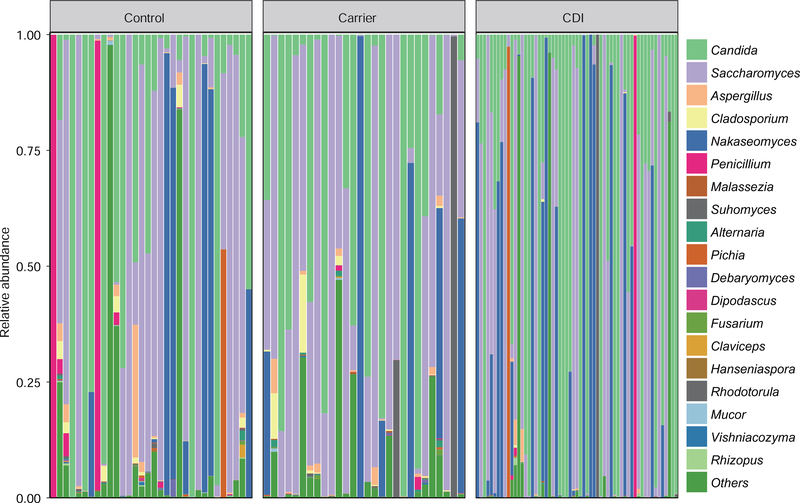
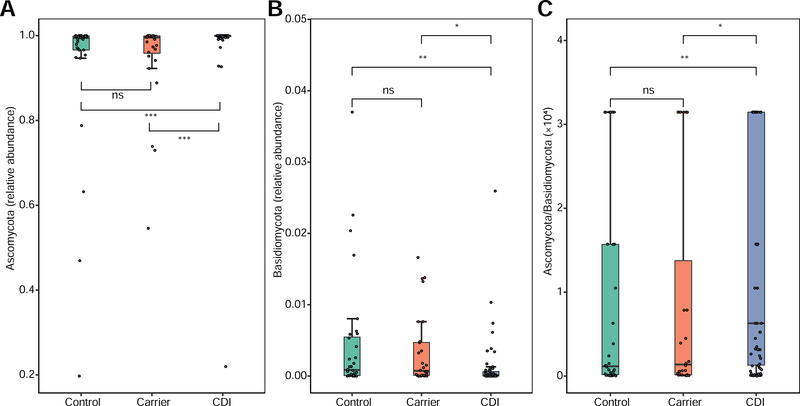
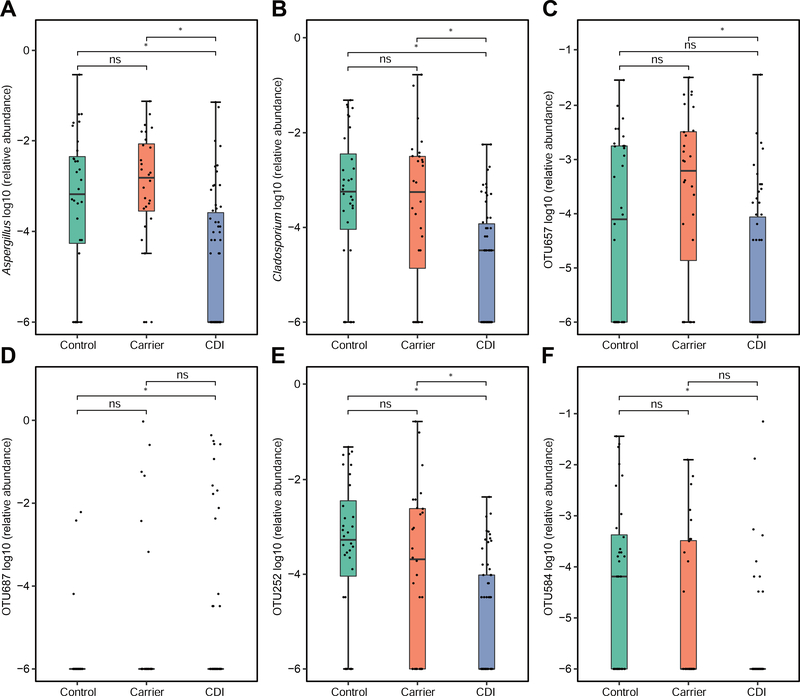
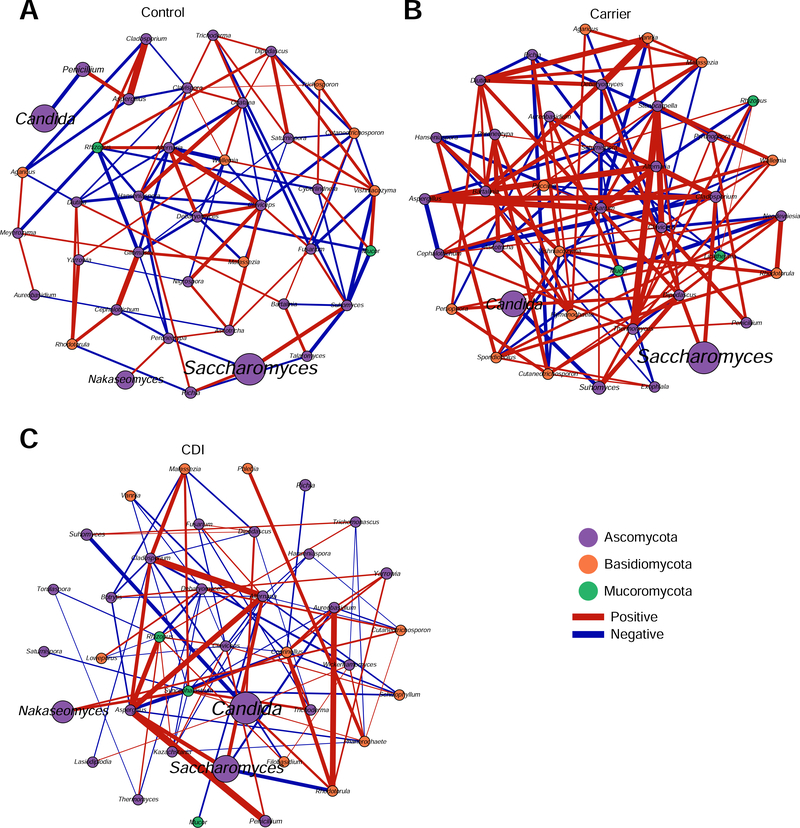
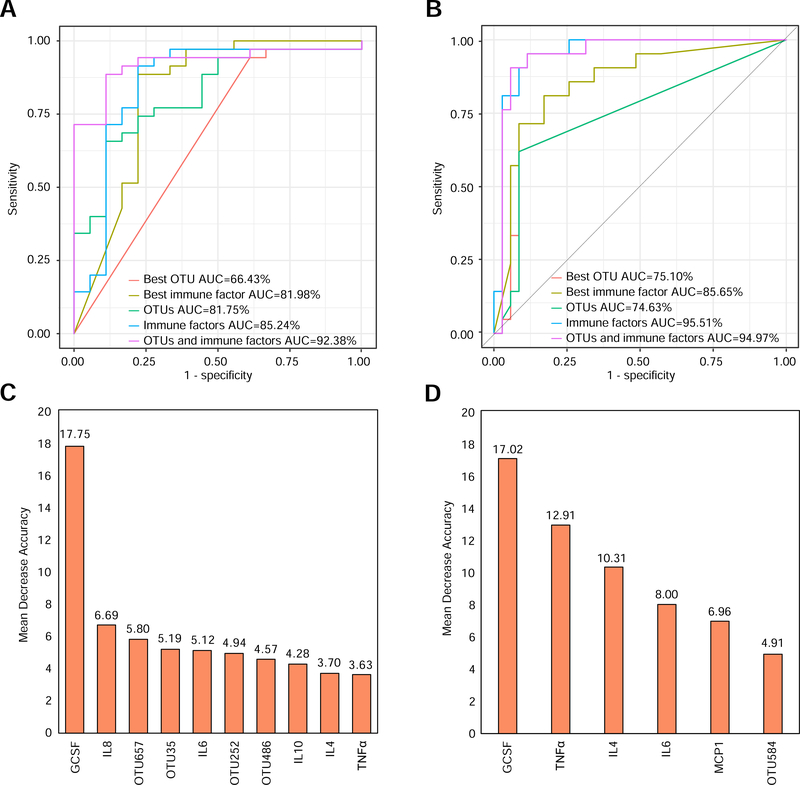
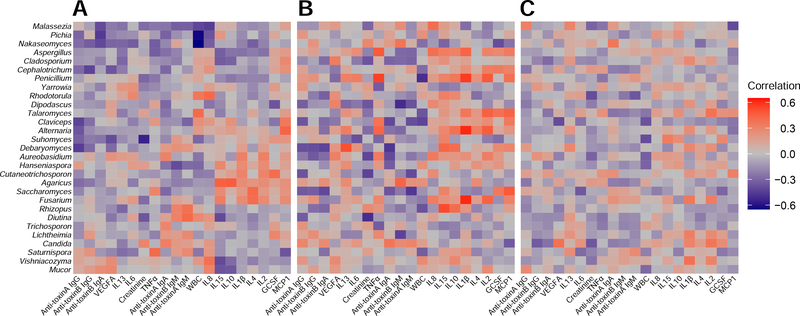
Results: Significant differences were observed in alpha and beta diversity between patients with CDI and Carrier (P < .05). Differential abundance analysis identified 2 genera (Cladosporium and Aspergillus) enriched in Carrier. The ratio of Ascomycota to Basidiomycota was dramatically higher in patients with CDI than in Carrier and Control (P < .05). Correlations between host immune factors and mycobiota features were weaker in patients with CDI than in Carrier. Using 4 fungal operational taxonomic units combined with 6 host immune markers in the random forest classifier can achieve very high performance (area under the curve ∼92.38%) in distinguishing patients with CDI from Carrier.
Conclusions: Our study provides specific markers of stool fungi combined with host immune factors to distinguish patients with CDI from Carrier. It highlights the importance of gut mycobiome in CDI, which may have been underestimated. Further studies on the diagnostic applications and therapeutic potentials of these findings are warranted.
Keywords: C difficile; Diagnostics; Gut Mycobiome; Immune Response.
Copyright © 2021 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Competing interests
No conflict of interest exists.
Figures
References
-
- McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 Update by the infectious diseases society of america (IDSA) and society for healthcare epidemiology of america (SHEA). Clin Infect Dis 2018;66:987–994. - PubMed
-
- Shim JK, Johnson S, Samore MH, et al. Primary symptomless colonisation by Clostridium difficile and decreased risk of subsequent diarrhoea. Lancet 1998;351:633–636. - PubMed
-
- Gerding DN, Johnson S. Management of Clostridium difficile infection: thinking inside and outside the box. Clin Infect Dis 2010;51:1306–1313. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
