

Gender Biases in Estimation of Others' Pain
- PMID: 33684539
- PMCID: PMC8827218
- DOI: 10.1016/j.jpain.2021.03.001
Gender Biases in Estimation of Others' Pain
Abstract
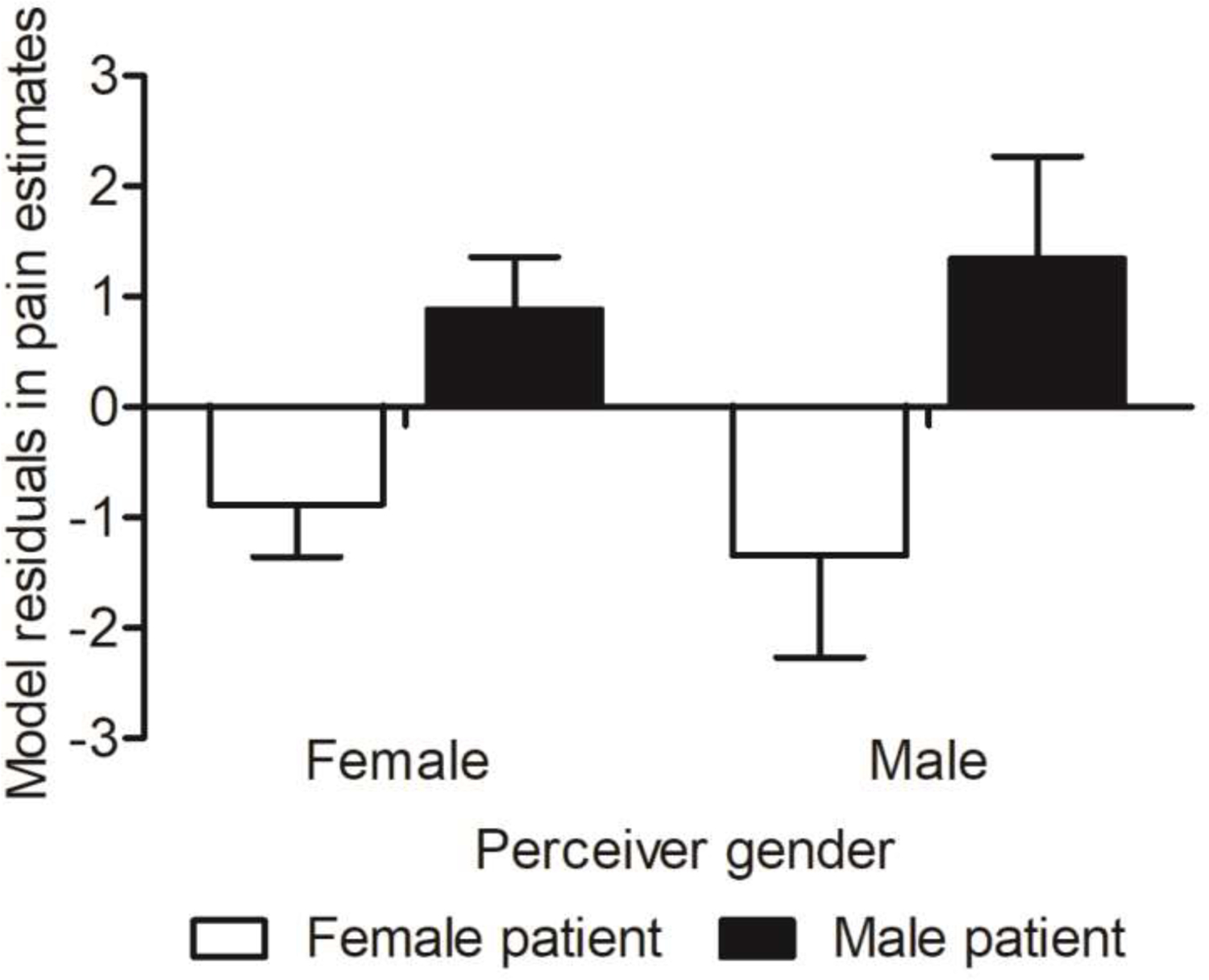
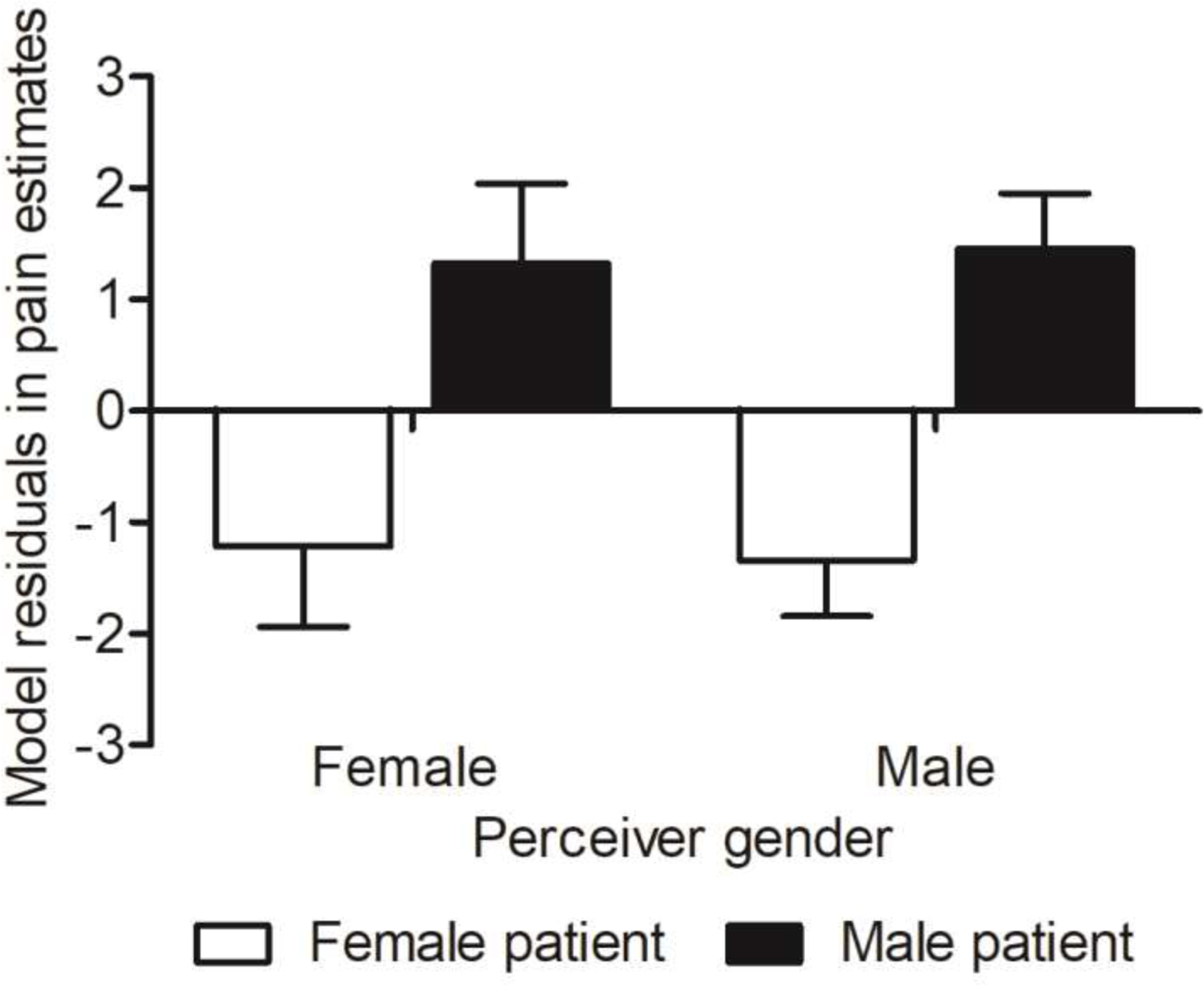
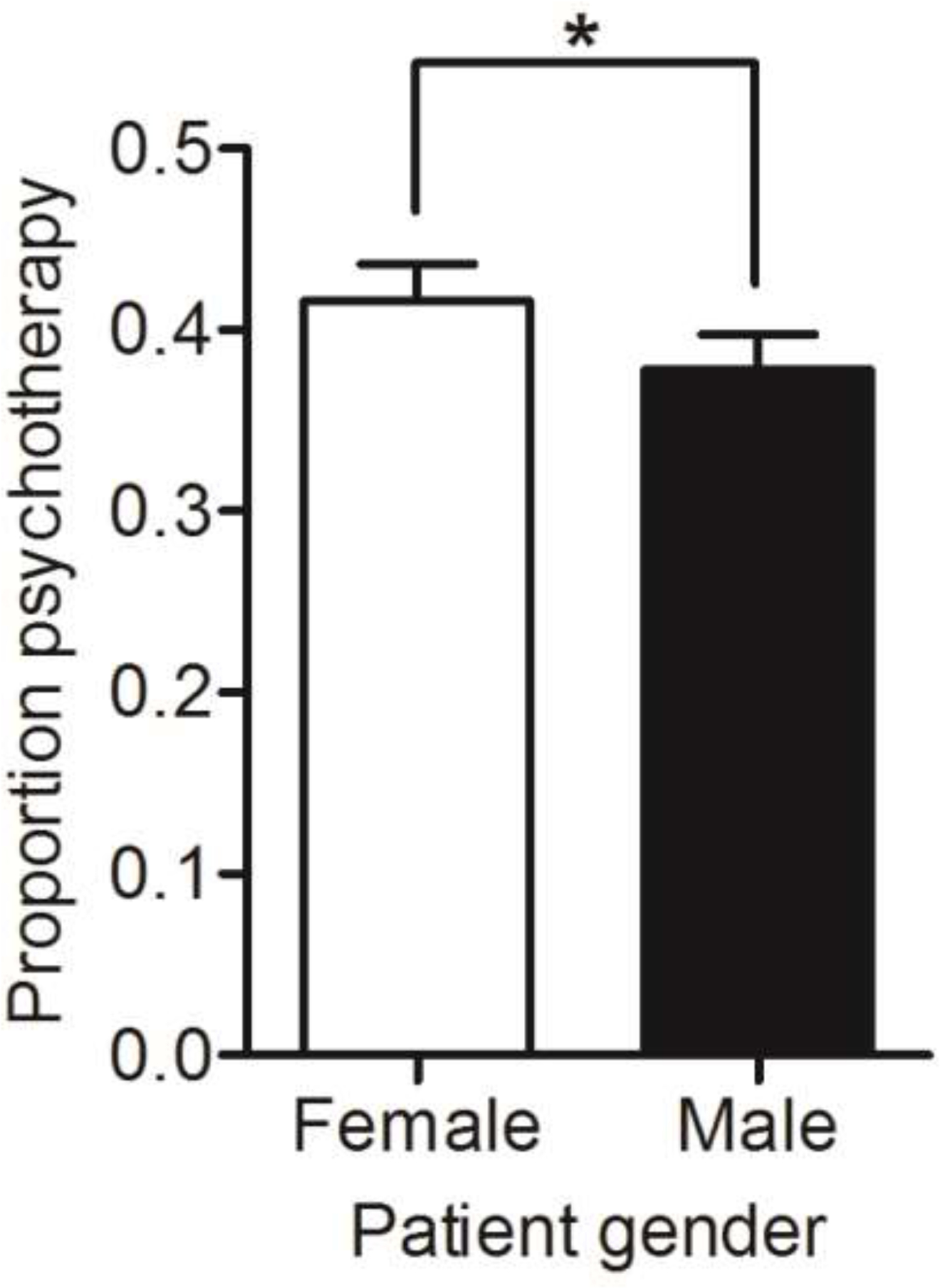
Caregiving and other interpersonal interactions often require accurate perception of others' pain from nonverbal cues, but perceivers may be subject to systematic biases based on gender, race, and other contextual factors. Such biases could contribute to systematic under-recognition and undertreatment of pain. In 2 experiments, we studied the impact of perceived patient sex on lay perceivers' pain estimates and treatment recommendations. In Experiment 1 (N = 50), perceivers viewed facial video clips of female and male patients in chronic shoulder pain and estimated patients' pain intensity. Multi-level linear modeling revealed that perceivers under-estimated female patients' pain compared with male patients, after controlling for patients' self-reported pain and pain facial expressiveness. Experiment 2 (N = 200) replicated these findings, and additionally found that 1) perceivers' pain-related gender stereotypes, specifically beliefs about typical women's vs. men's willingness to express pain, predicted pain estimation biases; and 2) perceivers judged female patients as relatively more likely to benefit from psychotherapy, whereas male patients were judged to benefit more from pain medicine. In both experiments, the gender bias effect size was on average 2.45 points on a 0-100 pain scale. Gender biases in pain estimation may be an obstacle to effective pain care, and experimental approaches to characterizing biases, such as the one we tested here, could inform the development of interventions to reduce such biases. Perspective: This study identifies a bias towards underestimation of pain in female patients, which is related to gender stereotypes. The findings suggest caregivers' or even clinicians' pain stereotypes are a potential target for intervention.
Keywords: Sex; gender bias; pain estimation; pain treatment recommendations; pain-related gender role expectation; stereotypes.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure: Multilevel General Linear Model code is available at:
Figures
References
-
- Bijlstra G, Holland RW, Wigboldus DH: The social face of emotion recognition: Evaluations versus stereotypes. J Exp Soc Psychol 46, 657–663, 2010.
-
- Boerner KE, Chambers CT, Gahagan J, Keogh E, Fillingim RB, Mogil JS: Conceptual complexity of gender and its relevance to pain. Pain 159: 2137–2141, 2018. - PubMed
-
- Broderick JE, Keefe FJ, Schneider S, Junghaenel DU, Bruckenthal P, Schwartz JE, Kaell AT, Caldwell DS, McKee D, Gould E: Cognitive behavioral therapy for chronic pain is effective, but for whom? Pain 157: 2115–2123, 2016. - PubMed
-
- Campbell C, Cramb G: ‘Nobody likes a back bore’–exploring lay perspectives of chronic pain: revealing the hidden voices of nonservice users. Scand J Caring Sci 22: 383–390, 2008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
