

Competing risks in patients with primary prevention implantable cardioverter-defibrillators: Global Electrical Heterogeneity and Clinical Outcomes study
- PMID: 33684549
- PMCID: PMC8169548
- DOI: 10.1016/j.hrthm.2021.03.006
Competing risks in patients with primary prevention implantable cardioverter-defibrillators: Global Electrical Heterogeneity and Clinical Outcomes study
Abstract
Background: Global electrical heterogeneity (GEH) is associated with sudden cardiac death in the general population. Its utility in patients with systolic heart failure who are candidates for primary prevention (PP) implantable cardioverter-defibrillators (ICDs) is unclear.
Objective: The purpose of this study was to investigate whether GEH is associated with sustained ventricular tachycardia/ventricular fibrillation leading to appropriate ICD therapies in patients with heart failure and PP ICDs.
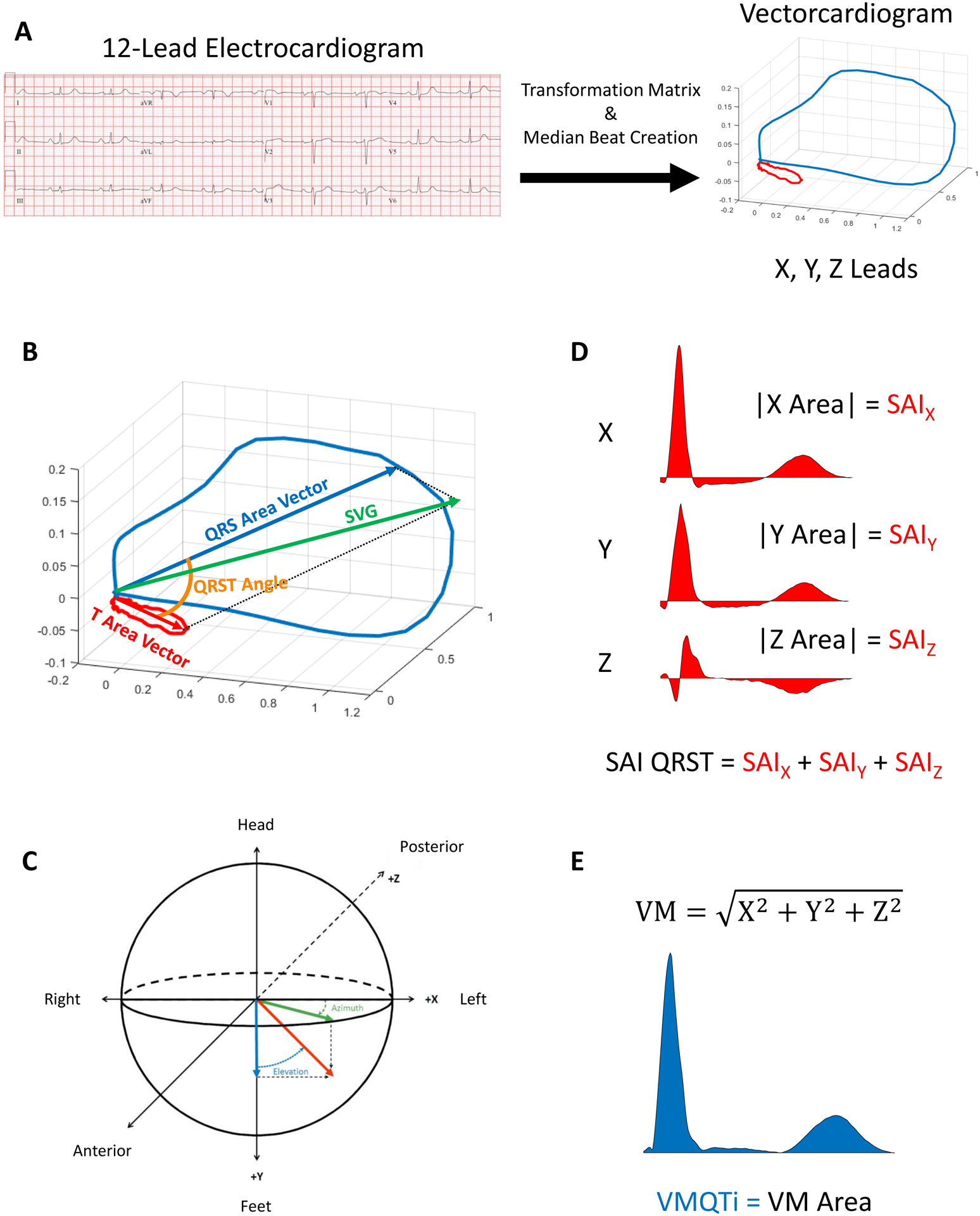
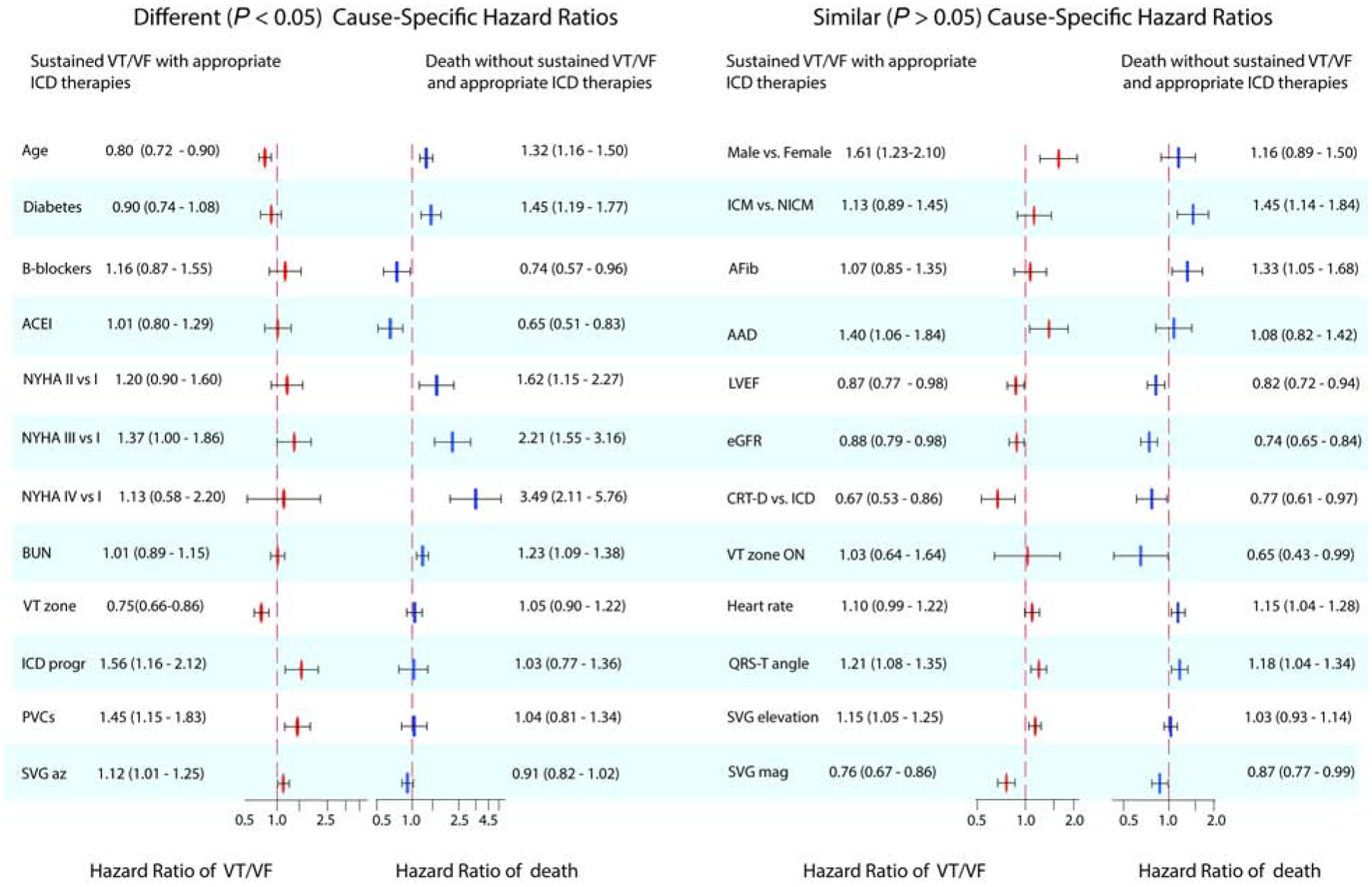
Methods: We conducted a multicenter retrospective cohort study. GEH was measured by spatial ventricular gradient (SVG) direction (azimuth and elevation) and magnitude, QRS-T angle, and sum absolute QRST integral on preimplant 12-lead electrocardiograms. Survival analysis using cause-specific hazard functions compared the strength of associations with 2 competing outcomes: sustained ventricular tachycardia/ventricular fibrillation leading to appropriate ICD therapies and all-cause death without appropriate ICD therapies.
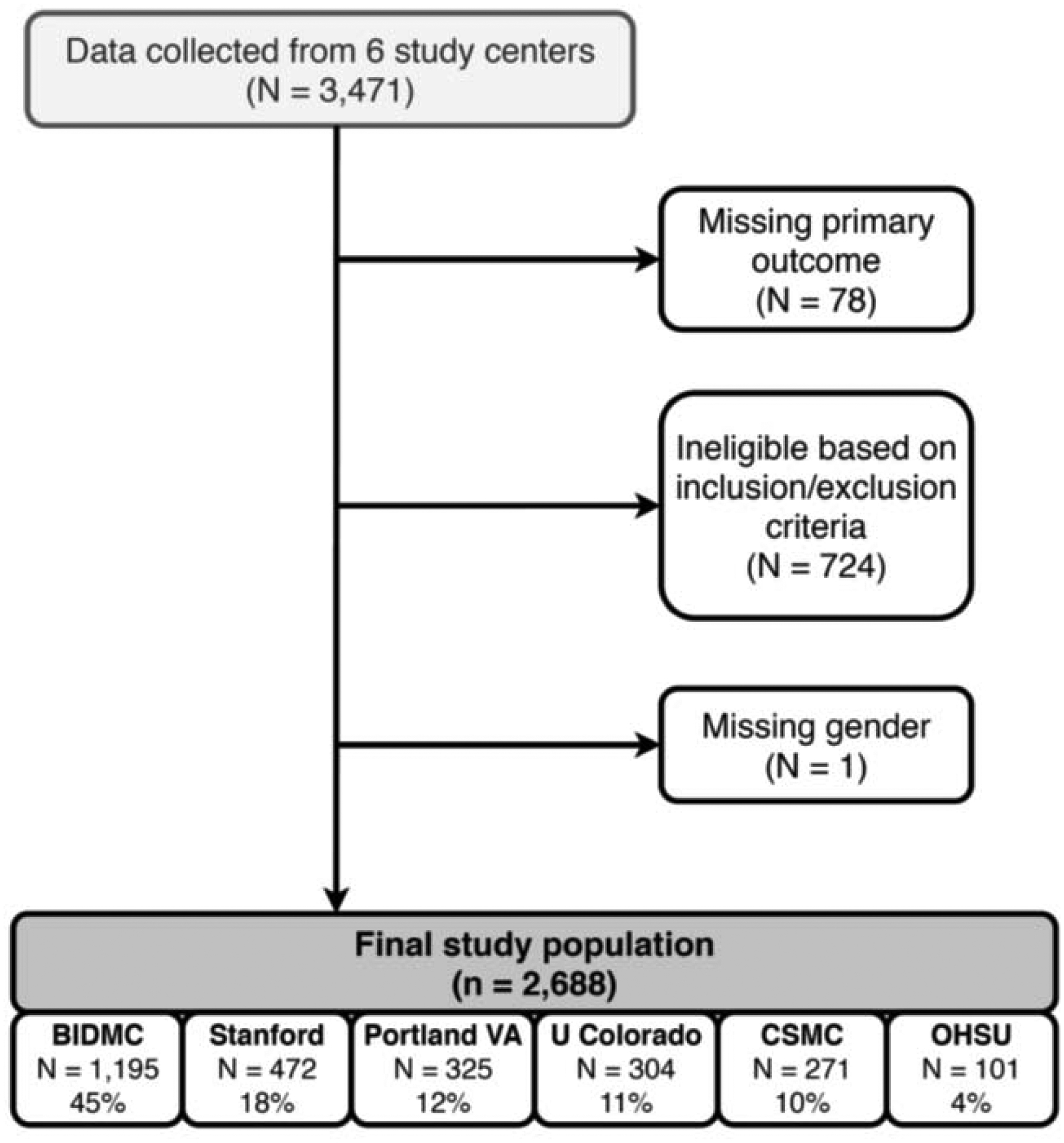
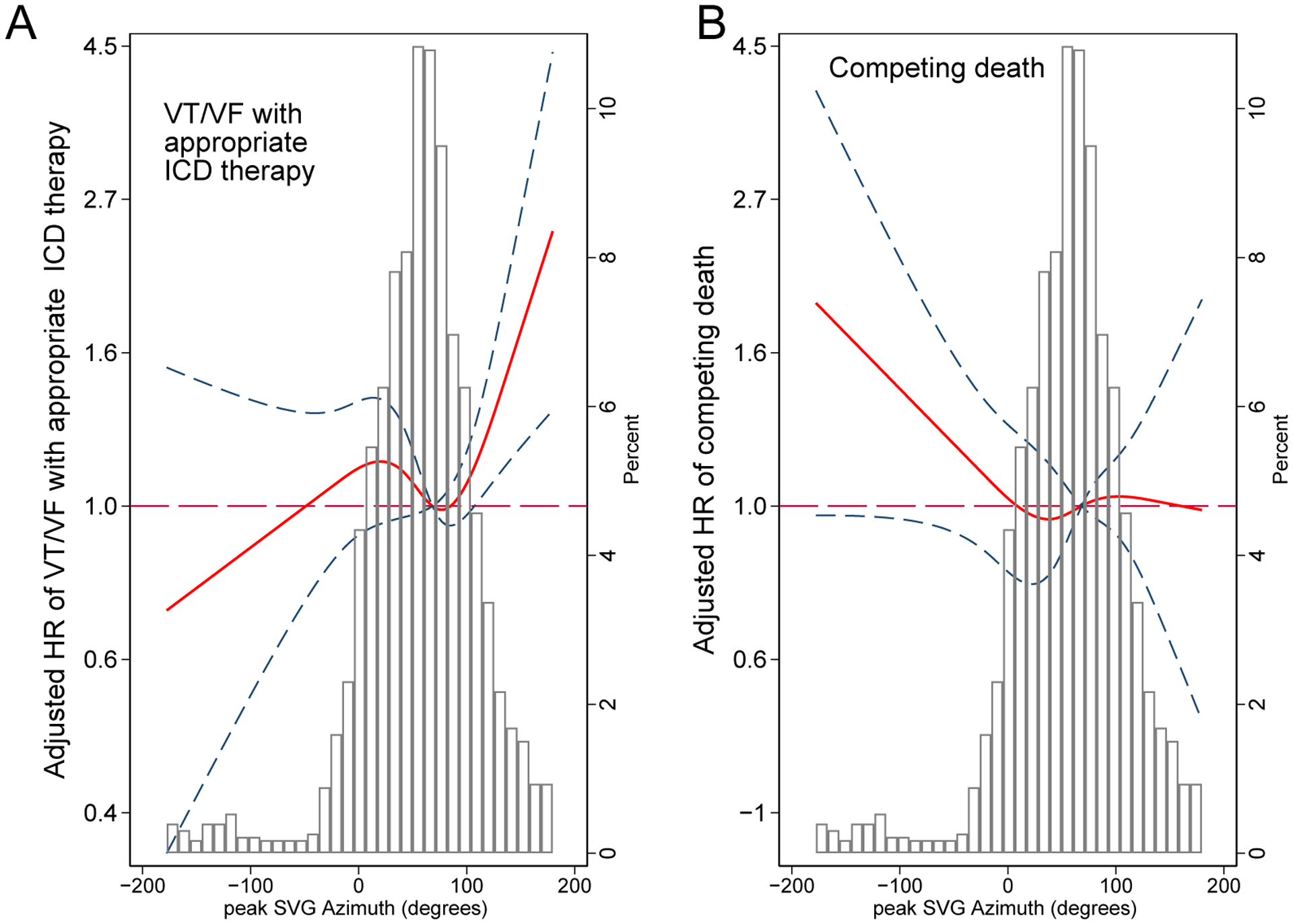
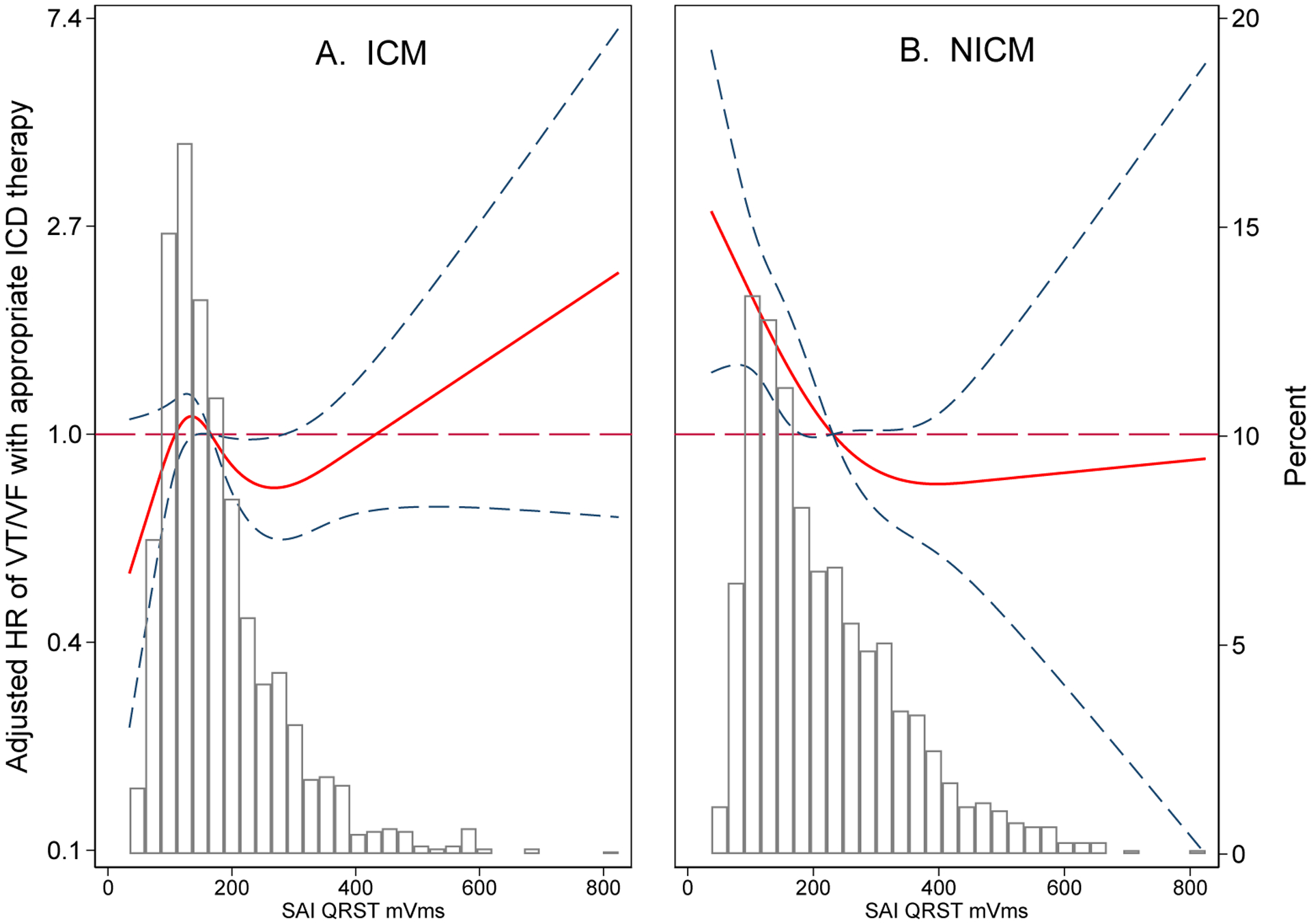
Results: We analyzed 2668 patients (mean age 63 ± 12 years; 624 (23%) female; 78% white; 43% nonischemic cardiomyopathy; left ventricular ejection fraction 28% ± 11% from 6 academic medical centers). After adjustment for demographic, clinical, device, and traditional electrocardiographic characteristics, SVG elevation (hazard ratio [HR] per 1SD 1.14; 95% confidence interval [CI] 1.04-1.25; P = .004), SVG azimuth (HR per 1SD 1.12; 95% CI 1.01-1.24; P = .039), SVG magnitude (HR per 1SD 0.75; 95% CI 0.66-0.85; P < .0001), and QRS-T angle (HR per 1SD 1.21; 95% CI 1.08-1.36; P = .001) were associated with appropriate ICD therapies. Sum absolute QRST integral had different associations in infarct-related cardiomyopathy (HR 1.29; 95% CI 1.04-1.60) and nonischemic cardiomyopathy (HR 0.78; 95% CI 0.62-0.96) (Pinteraction = .022).
Conclusion: In patients with PP ICDs, GEH is independently associated with appropriate ICD therapies. The SVG vector points in distinctly different directions in patients with 2 competing outcomes.
Keywords: Competing risk; Global electrical heterogeneity; Heart failure; Implantable cardioverter-defibrillators; Ventricular tachycardia/Ventricular fibrillation.
Copyright © 2021 Heart Rhythm Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 2018;15:e190–e252. - PubMed
-
- Kober L, Thune JJ, Nielsen JC, et al. Defibrillator Implantation in Patients with Nonischemic Systolic Heart Failure. N Engl J Med 2016;375:1221–1230. - PubMed
-
- Burch GE, Abildskov JA, Cronvich JA. A Study of the Spatial Vectorcardiogram of the Ventricular Gradient. Circulation 1954;9:267–275. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
