

Factors predicting long-term outcomes of early-stage hepatocellular carcinoma after primary curative treatment: the role of surgical or nonsurgical methods
- PMID: 33685409
- PMCID: PMC7941925
- DOI: 10.1186/s12885-021-07948-9
Factors predicting long-term outcomes of early-stage hepatocellular carcinoma after primary curative treatment: the role of surgical or nonsurgical methods
Abstract
Background: We quantified the elusive effects of putative factors on the clinical course of early hepatocellular carcinoma (HCC) after primary surgical or nonsurgical curative treatment.
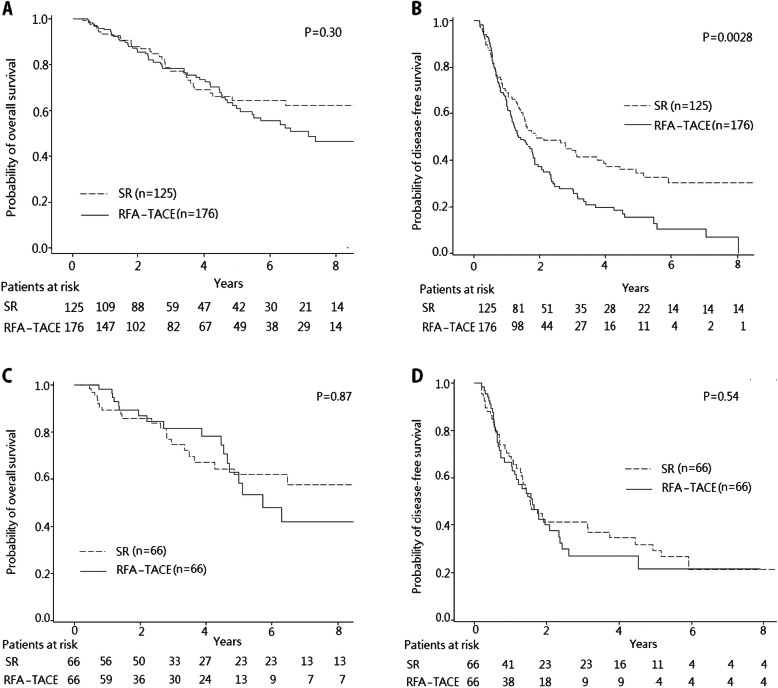
Methods: Patients with newly diagnosed early HCC who received surgical resection (SR) or percutaneous radiofrequency ablation (RFA) with or without transcatheter arterial chemoembolization (TACE) from January 2003 to December 2016 were enrolled. The cumulative overall survival (OS) and disease-free survival (DFS) rates were compared. A polytomous logistic regression was used to estimate factors for early and late recurrence. Independent predictors of OS were identified using Cox proportional hazard regression.
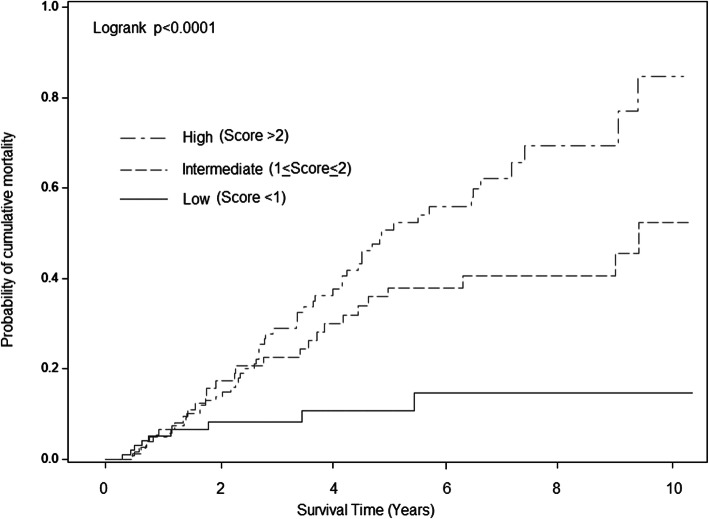
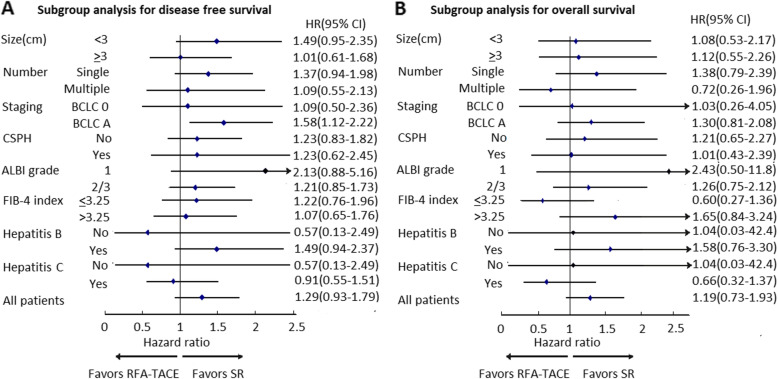
Results: One hundred twenty-five patients underwent SR, and 176 patients underwent RFA, of whom 72 were treated with TACE followed by RFA. Neither match analysis based on propensity score nor multiple adjustment regression yielded a significant difference in DFS and OS between the two groups. Multivariate analysis showed high AFP (> 20 ng/mL), and multinodularity significantly increased risk of early recurrence (< 1 year). In contrast, hepatitis B virus, hepatitis C virus and multinodularity were significantly associated with late recurrence (> 1 year). Multivariate Cox regression with recurrent events as time-varying covariates identified older age (HR = 1.55, 95% CI:1.01-2.36), clinically significant portal hypertension (CSPH) (HR = 1.97, 95% CI:1.26-3.08), early recurrence (HR = 6.62, 95% CI:3.79-11.6) and late recurrence (HR = 3.75, 95% CI:1.99-7.08) as independent risk factors of mortality. A simple risk score showed fair calibration and discrimination in early HCC patients after primary curative treatment. In the Barcelona Clinic Liver Cancer (BCLC) stage A subgroup, SR significantly improved DFS compared to RFA with or without TACE.
Conclusion: Host and tumor factors rather than the initial treatment modalities determine the outcomes of early HCC after primary curative treatment. Statistical models based on recurrence types can predict early HCC prognosis but further external validation is necessary.
Keywords: Early hepatocellular carcinoma; Prognosis; Propensity score matching; Radiofrequency ablation; Surgical resection; Transcatheter arterial chemoembolization.
Conflict of interest statement
Ming-Jeng Kuo, Lein-Ray Mo, Chi-Ling Chen declare that they have no conflict of interest.
Figures
References
-
- Chan AWH, Zhong J, Berhane S, Toyoda H, Cucchetti A, Shi K, Tada T, Chong CCN, Xiang BD, Li LQ, et al. Development of pre and post-operative models to predict early recurrence of hepatocellular carcinoma after surgical resection. J Hepatol. 2018;69(6):1284–1293. doi: 10.1016/j.jhep.2018.08.027. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
