

Taking a step down on the reconstruction ladder for head and neck reconstruction during the COVID-19 pandemic
- PMID: 33685447
- PMCID: PMC7938274
- DOI: 10.1186/s12893-021-01134-1
Taking a step down on the reconstruction ladder for head and neck reconstruction during the COVID-19 pandemic
Abstract
Background: Most of the head and neck cancers are time-critical and need urgent surgical treatment. Our unit is one of the departments in the region, at the forefront in treating head and neck cancers in Pakistan. We have continued treating these patients in the COVID-19 pandemic with certain modified protocols. The objective of this study is to share our experience and approach towards head and neck reconstruction during the COVID-19 pandemic.
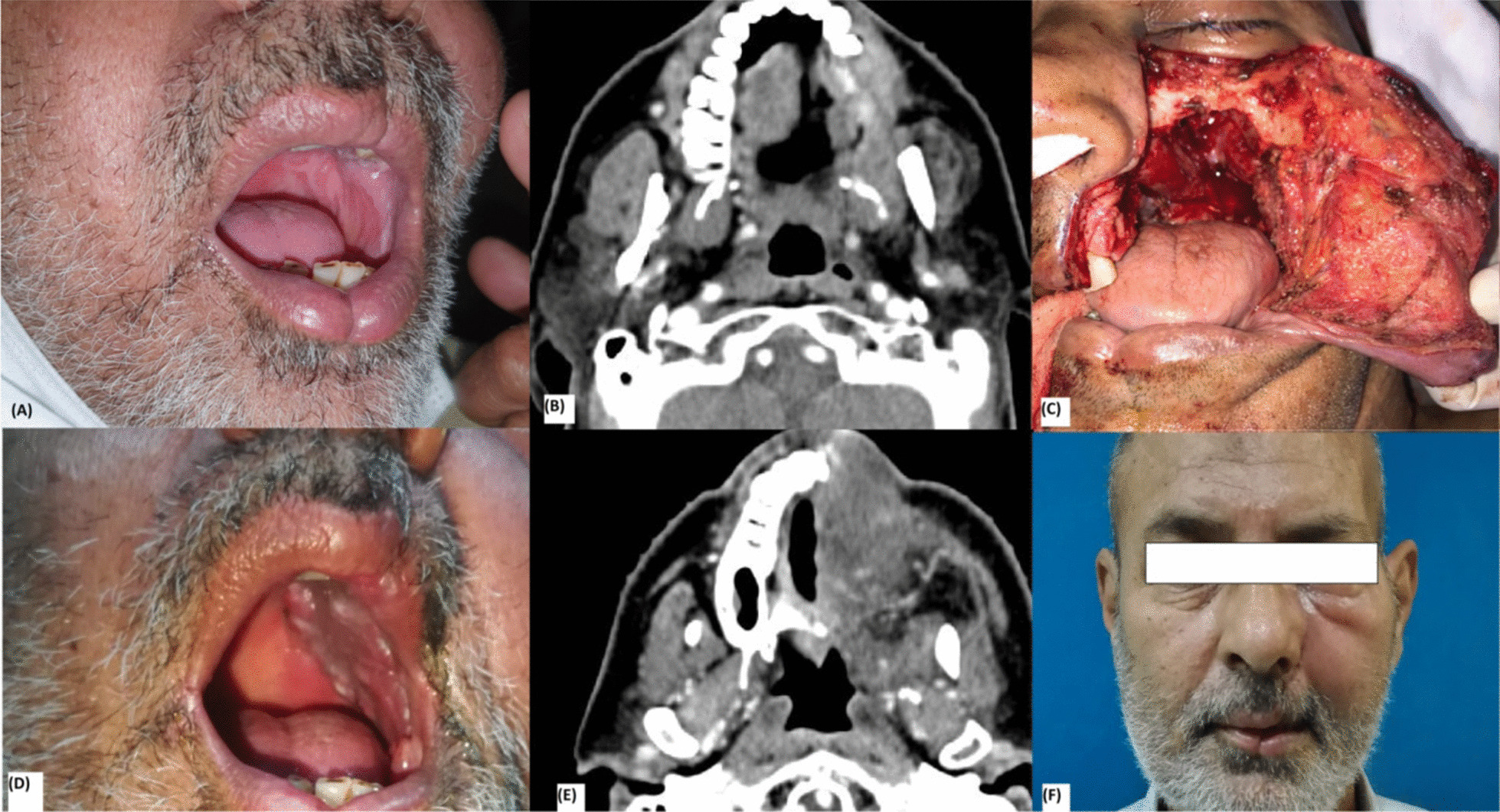
Results: There were a total of 31 patients, 20 (64.5%) were males and 11 (35.4%) patients were females. The mean age of patients was 52 years. Patients presented with different pathologies, i.e. Squamous cell carcinoma n = 26 (83.8%), mucoepidermoid carcinoma n = 2 (6.4%), adenoid cystic carcinoma n = 2 (6.4%) and mucormycosis n = 1 (3%). The reconstruction was done with loco-regional flaps like temporalis muscle flap n = 12 (38.7%), Pectoralis major myocutaneous flap n = 8 (25.8%), supraclavicular artery flap n = 10 (32.2%) and combination of fore-head, temporalis major and cheek rotation flaps n = 1 (3%). Defects involved different regions like maxilla n = 11 (35.4%), buccal mucosa n = 6 (19.3%), tongue with floor of mouth n = 6 (19.3%), mandible n = 4 (12.9%), parotid gland, mastoid n = 3 (9.6%) and combination of defects n = 1 (3%). Metal reconstruction plate was used in 3 (9.6%) patients with mandibular defects. All flaps survived, with the maximum follow-up of 8 months and minimum follow-up of 6 months.
Conclusion: Pedicled flaps are proving as the workhorse for head and neck reconstruction in unique global health crisis. Vigilant use of proper PPE and adherence to the ethical principles proves to be the only shield that will benefit patients, HCW and health system.
Keywords: Head and neck reconstruction; Pedicled flaps in free flap era; Reconstruction in COVID 19 pandemic.
Conflict of interest statement
There are no competing interests.
Figures







References
-
- World Health Organization. Coronavirus disease 2019 (COVID-2019) Situation Report-51. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2....
-
- Coronavirus Disease 2019: For Healthcare Professionals. https://www.cdc.gov/coronavirus/2019-nCoV/hcp/index.html.
-
- CMS Adult Elective Surgery and Procedures Recommendations. https://cms.gov/files/document/covid-elective-surgery-recommendations.pdf.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
