

Quantifying the potential value of antigen-detection rapid diagnostic tests for COVID-19: a modelling analysis
- PMID: 33685466
- PMCID: PMC7939929
- DOI: 10.1186/s12916-021-01948-z
Quantifying the potential value of antigen-detection rapid diagnostic tests for COVID-19: a modelling analysis
Abstract
Background: Testing plays a critical role in treatment and prevention responses to the COVID-19 pandemic. Compared to nucleic acid tests (NATs), antigen-detection rapid diagnostic tests (Ag-RDTs) can be more accessible, but typically have lower sensitivity and specificity. By quantifying these trade-offs, we aimed to inform decisions about when an Ag-RDT would offer greater public health value than reliance on NAT.
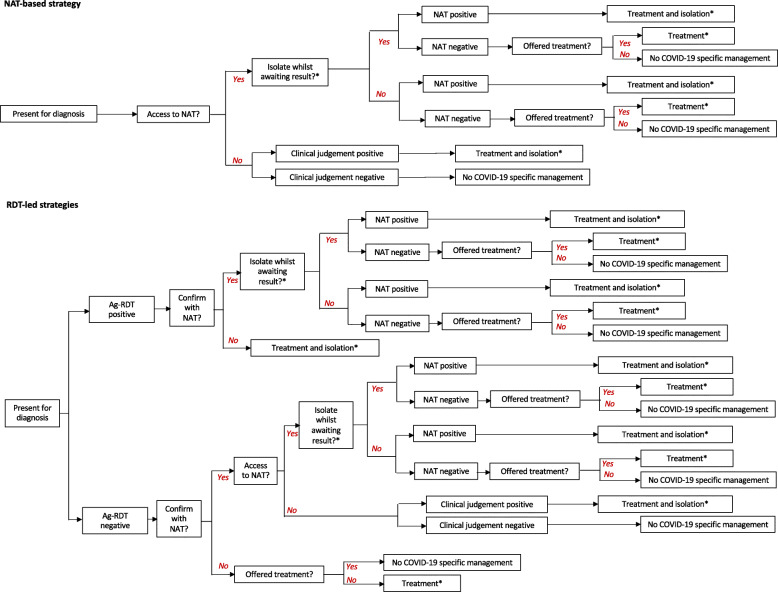
Methods: Following an expert consultation, we selected two use cases for analysis: rapid identification of people with COVID-19 amongst patients admitted with respiratory symptoms in a 'hospital' setting and early identification and isolation of people with mildly symptomatic COVID-19 in a 'community' setting. Using decision analysis, we evaluated the health system cost and health impact (deaths averted and infectious days isolated) of an Ag-RDT-led strategy, compared to a strategy based on NAT and clinical judgement. We adopted a broad range of values for 'contextual' parameters relevant to a range of settings, including the availability of NAT and the performance of clinical judgement. We performed a multivariate sensitivity analysis to all of these parameters.
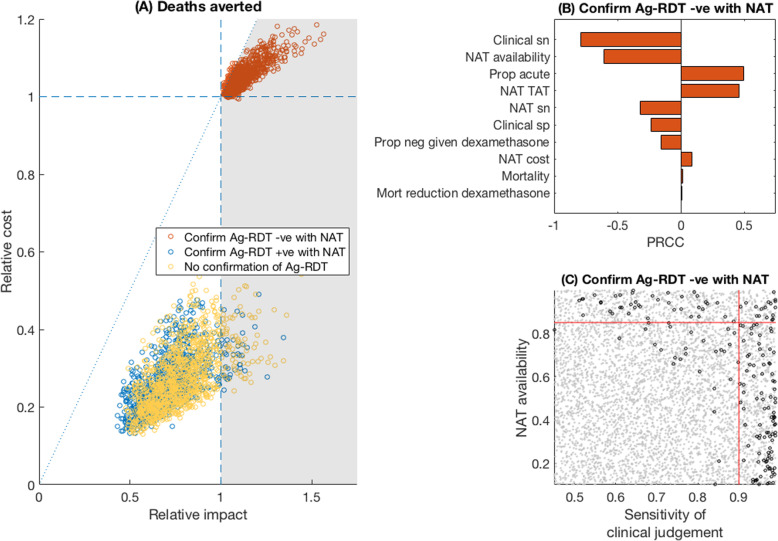
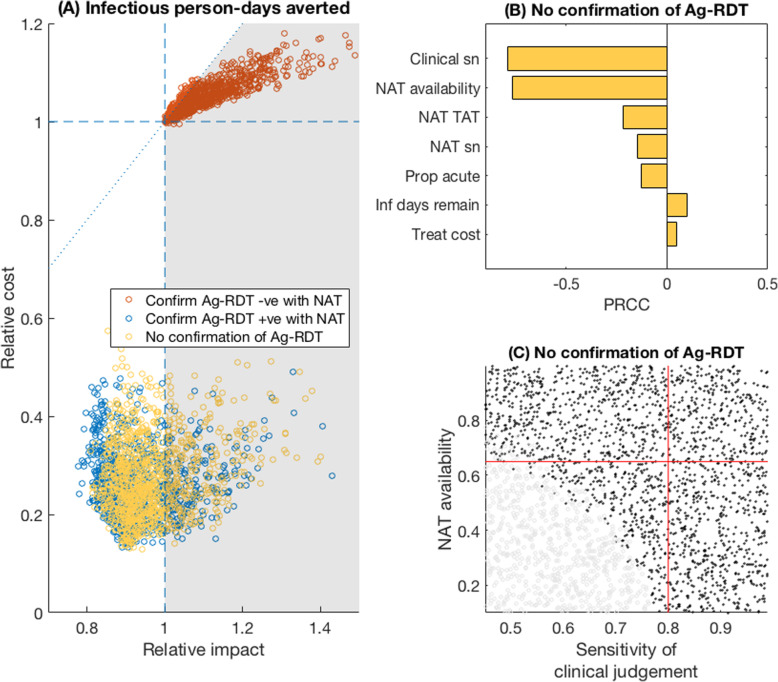
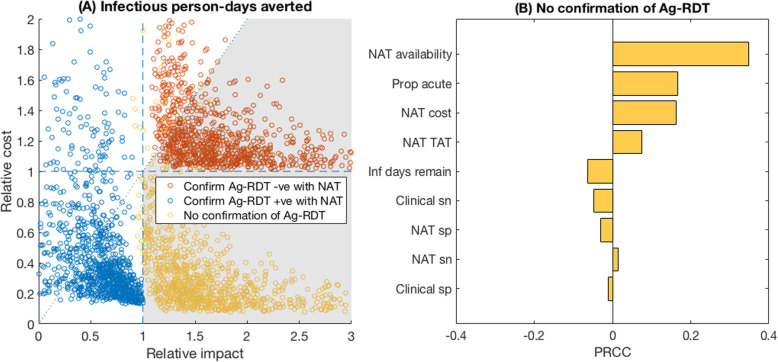
Results: In a hospital setting, an Ag-RDT-led strategy would avert more deaths than a NAT-based strategy, and at lower cost per death averted, when the sensitivity of clinical judgement is less than 90%, and when NAT results are available in time to inform clinical decision-making for less than 85% of patients. The use of an Ag-RDT is robustly supported in community settings, where it would avert more transmission at lower cost than relying on NAT alone, under a wide range of assumptions.
Conclusions: Despite their imperfect sensitivity and specificity, Ag-RDTs have the potential to be simultaneously more impactful, and have a lower cost per death and infectious person-days averted, than current approaches to COVID-19 diagnostic testing.
Keywords: Antigen; COVID-19; Rapid diagnostic tests.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organisation . WHO COVID-19 Preparedness and Response Progress Report - 1 February to 30 June 2020. Geneva: WHO; 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
