

De novo TRPV4 Leu619Pro variant causes a new channelopathy characterised by giant cell lesions of the jaws and skull, skeletal abnormalities and polyneuropathy
- PMID: 33685999
- PMCID: PMC8867273
- DOI: 10.1136/jmedgenet-2020-107427
De novo TRPV4 Leu619Pro variant causes a new channelopathy characterised by giant cell lesions of the jaws and skull, skeletal abnormalities and polyneuropathy
Abstract
Background: Pathogenic germline variants in Transient Receptor Potential Vanilloid 4 Cation Channel (TRPV4) lead to channelopathies, which are phenotypically diverse and heterogeneous disorders grossly divided in neuromuscular disorders and skeletal dysplasia. We recently reported in sporadic giant cell lesions of the jaws (GCLJs) novel, somatic, heterozygous, gain-of-function mutations in TRPV4, at Met713.
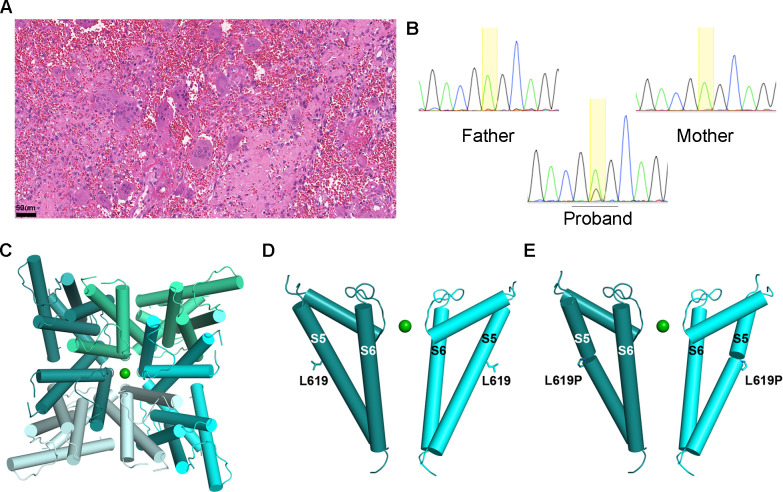
Methods: Here we report two unrelated women with a de novo germline p.Leu619Pro TRPV4 variant and an overlapping systemic disorder affecting all organs individually described in TRPV4 channelopathies.
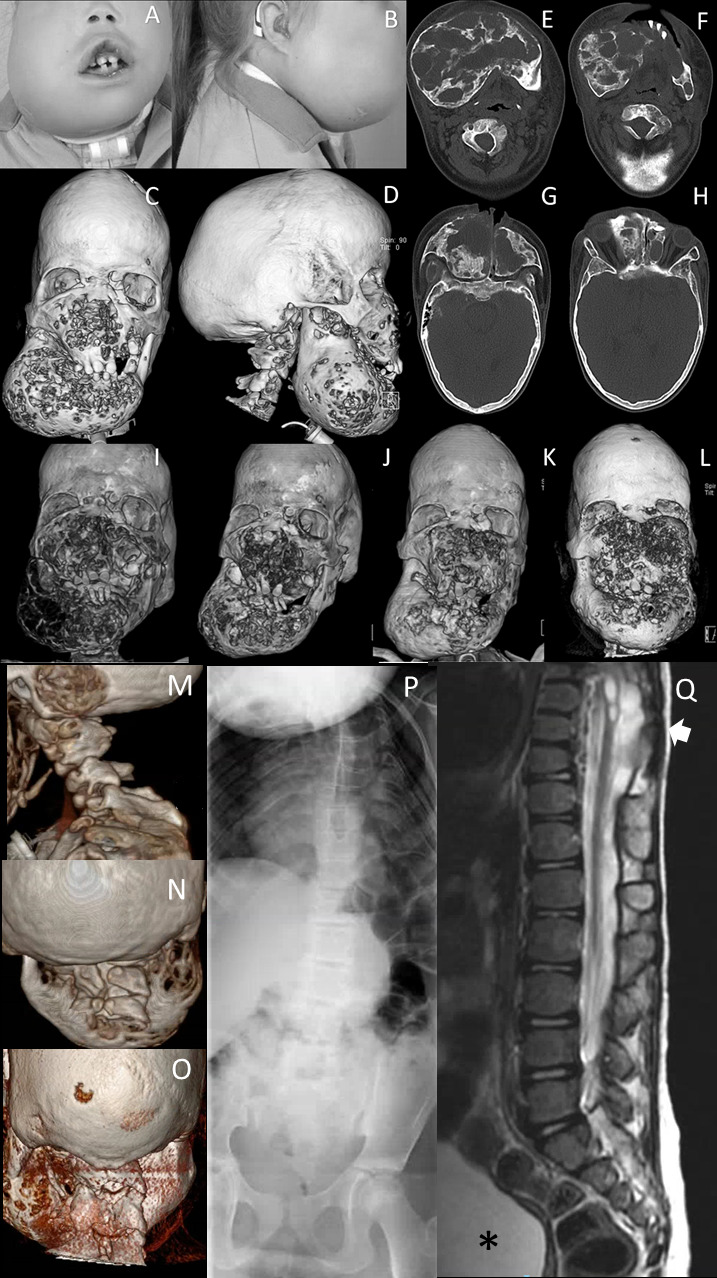
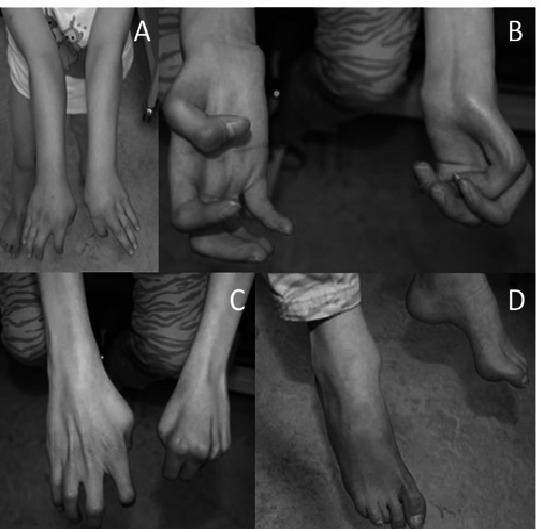
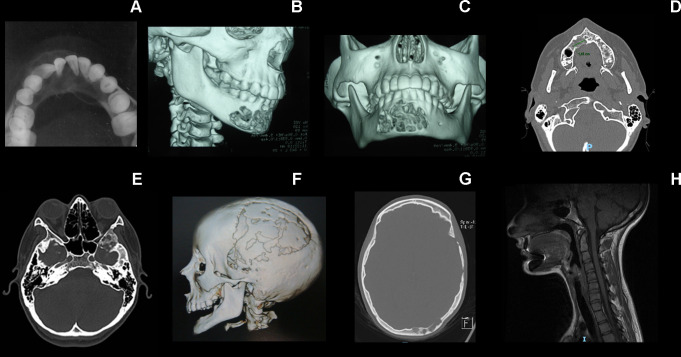
Results: From an early age, both patients had several lesions of the nervous system including progressive polyneuropathy, and multiple aggressive giant cell-rich lesions of the jaws and craniofacial/skull bones, and other skeletal lesions. One patient had a relatively milder disease phenotype possibly due to postzygotic somatic mosaicism. Indeed, the TRPV4 p.Leu619Pro variant was present at a lower frequency (variant allele frequency (VAF)=21.6%) than expected for a heterozygous variant as seen in the other proband, and showed variable regional frequency in the GCLJ (VAF ranging from 42% to 10%). In silico structural analysis suggests that the gain-of-function p.Leu619Pro alters the ion channel activity leading to constitutive ion leakage.
Conclusion: Our findings define a novel polysystemic syndrome due to germline TRPV4 p.Leu619Pro and further extend the spectrum of TRPV4 channelopathies. They further highlight the convergence of TRPV4 mutations on different organ systems leading to complex phenotypes which are further mitigated by possible post-zygotic mosaicism. Treatment of this disorder is challenging, and surgical intervention of the GCLJ worsens the lesions, suggesting the future use of MEK inhibitors and TRPV4 antagonists as therapeutic modalities for unmet clinical needs.
Keywords: genetics; medical; nervous system diseases; pathology; plastic; stomatognathic diseases; surgery.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: RG and CCG are research fellows at the National Council for Scientific and Technological Development, Brazil.
Figures
References
-
- Mortier GR, Cohn DH, Cormier-Daire V, Hall C, Krakow D, Mundlos S, Nishimura G, Robertson S, Sangiorgi L, Savarirayan R, Sillence D, Superti-Furga A, Unger S, Warman ML. Nosology and classification of genetic skeletal disorders: 2019 revision. Am J Med Genet A 2019;179:2393–419. 10.1002/ajmg.a.61366 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources