

Histopathology of Non-IBD Colitis. A practical approach from the Italian Group for the study of the gastrointestinal tract (GIPAD)
- PMID: 33686310
- PMCID: PMC8138693
- DOI: 10.32074/1591-951X-234
Histopathology of Non-IBD Colitis. A practical approach from the Italian Group for the study of the gastrointestinal tract (GIPAD)
Abstract
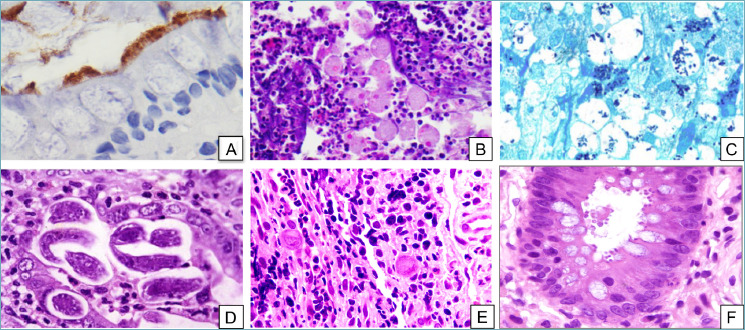
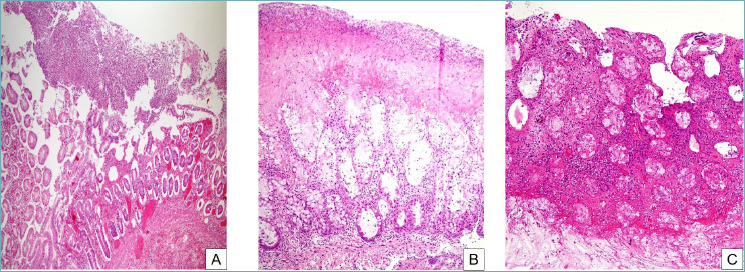
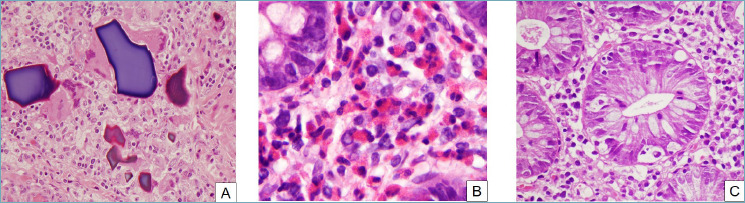
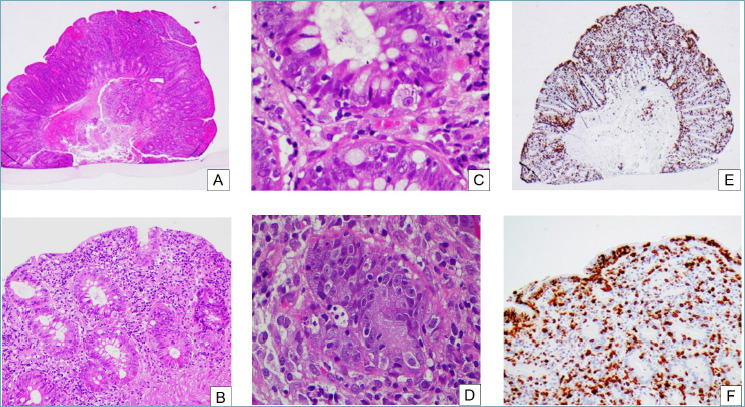
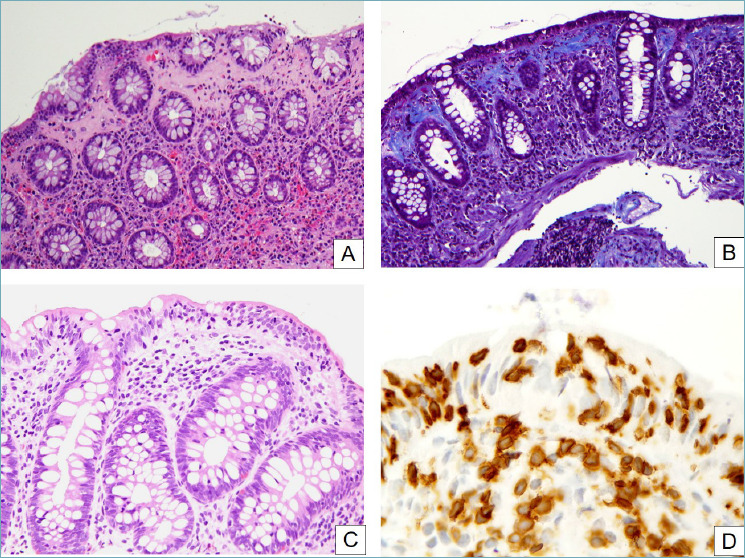
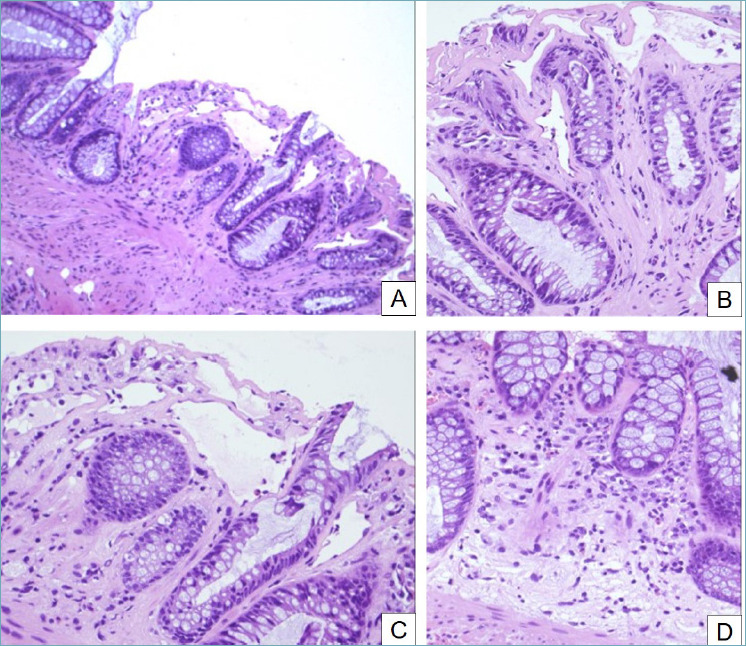
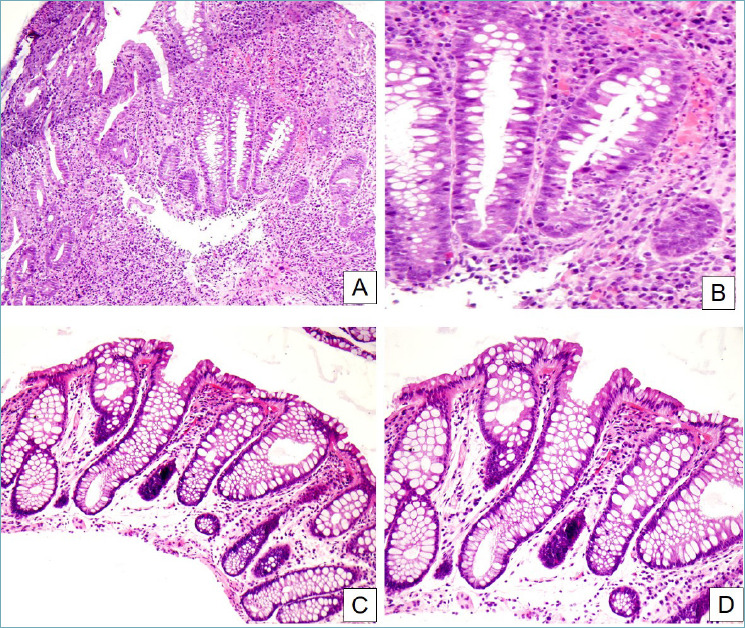
Non-IBD colitides (NIBDC) are intestinal diseases clinically and endoscopically overlapping with Inflammatory Bowel Diseases (IBD), sometimes with a similar histological picture. NIBDC include entities such as infectious colitis, ischemic colitis, pseudomembranous colitis, eosinophilic colitis, autoimmune enterocolitis, segmental colitis associated with diverticulosis, drug-induced colitis, radiation-induced colitis, diversion colitis, and microscopic colitis, this last including two entities: collagenous and lymphocytic colitis. The knowledge of the most useful histological features and the main clinical data for each entity is mandatory in daily clinical practice, for correct pathological diagnosis and clinical management.
Keywords: colitis; drug-induced colitis; infectious colitis; ischemic colitis; microscopic colitis.
Copyright © 2021 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures
References
-
- Schofield JB, Haboubi N. Histopathological mimics of inflammatory bowel disease. Inflamm Bowel Dis 2020. June 18;26(7):994-1009. https://doi.org/10.1093/ibd/izz232 10.1093/ibd/izz232 - DOI - PubMed
-
- Villanacci V, Reggiani-Bonetti L, Caprioli F, et al. Histopathology of inflammatory bowel disease - Position statement of the Pathologists of the Italian Group for the Study of Inflammatory Bowel Disease (IG-IBD) and Italian Group of Gastrointestinal Pathologists (GIPAD-SIAPEC). Dig Liv Dis 2020;52:262-7. https://doi.org/10.1016/j.dld.2019.11.005 10.1016/j.dld.2019.11.005 - DOI - PubMed
-
- Villanacci V, Reggiani-Bonetti L, Salviato T, et al. Histopathology of IBD Colitis. A practical approach from the pathologists of the Italian Group for the study of the gastrointestinal tract (GIPAD). Pathologica 2021;113:39-53. https://doi.org/10.32074/1591-951X-235 10.32074/1591-951X-235 - DOI - PMC - PubMed
-
- Leder K, Torresi J, Brownstein JS, et al. Travel-associated illness trends and clusters, 2000-2010. Emerg Infect Dis 2015;19:1049-73. https://doi.org/10.3201/eid1907.121573 10.3201/eid1907.121573 - DOI - PMC - PubMed
-
- Lamps LW. Update on infectious enterocolitis and the diseases that they mimic. Histopathology 2015;66:3-14. https://doi.org/10.1111/his.12582 10.1111/his.12582 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
