

Multilevel Factors Associated With More Intensive Use of Radioactive Iodine for Low-Risk Thyroid Cancer
- PMID: 33687063
- PMCID: PMC8118575
- DOI: 10.1210/clinem/dgab139
Multilevel Factors Associated With More Intensive Use of Radioactive Iodine for Low-Risk Thyroid Cancer
Abstract
Context: The use of radioactive iodine (RAI) for low-risk thyroid cancer is common, and variation in its use exists, despite the lack of benefit for low-risk disease and potential harms and costs.
Objective: To simultaneously assess patient- and physician-level factors associated with patient-reported receipt of RAI for low-risk thyroid cancer.
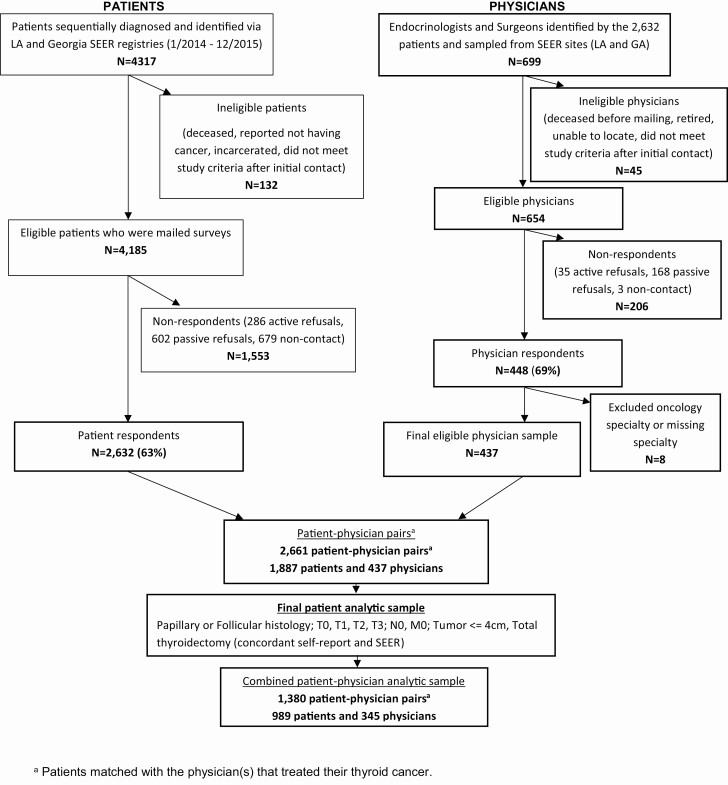
Methods: This population-based survey study of patients with newly diagnosed differentiated thyroid cancer identified via the Surveillance Epidemiology and End Results (SEER) registries of Georgia and Los Angeles County included 989 patients with low-risk thyroid cancer, linked to 345 of their treating general surgeons, otolaryngologists, and endocrinologists. We assessed the association of physician- and patient-level factors with patient-reported receipt of RAI for low-risk thyroid cancer.
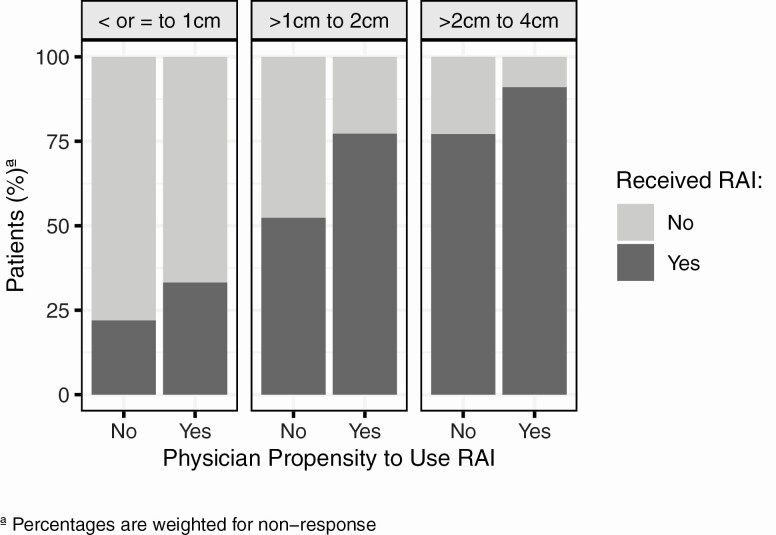
Results: Among this sample, 48% of patients reported receiving RAI, and 23% of their physicians reported they would use RAI for low-risk thyroid cancer. Patients were more likely to report receiving RAI if they were treated by a physician who reported they would use RAI for low-risk thyroid cancer compared with those whose physician reported they would not use RAI (adjusted OR: 1.84; 95% CI, 1.29-2.61). The odds of patients reporting they received RAI was 55% lower among patients whose physicians reported they saw a higher volume of patients with thyroid cancer (40+ vs 0-20) (adjusted OR: 0.45; 0.30-0.67).
Conclusions: Physician perspectives and attitudes about using RAI, as well as patient volume, influence RAI use for low-risk thyroid cancer. Efforts to reduce overuse of RAI in low-risk thyroid cancer should include interventions targeted toward physicians, in addition to patients.
Keywords: decision making; overtreatment; radioactive iodine; thyroid cancer.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Endocrine Society. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26(1):1-133. - PMC - PubMed
-
- Tuttle RM, Tala H, Shah J, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. 2010;20(12):1341-1349. - PMC - PubMed
-
- Cooper DS, Doherty GM, Haugen BR, et al. ; American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer . Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167-1214. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
