

Prevalence of Central Nervous System-Active Polypharmacy Among Older Adults With Dementia in the US
- PMID: 33687462
- PMCID: PMC7944381
- DOI: 10.1001/jama.2021.1195
Prevalence of Central Nervous System-Active Polypharmacy Among Older Adults With Dementia in the US
Abstract
Importance: Community-dwelling older adults with dementia have a high prevalence of psychotropic and opioid use. In these patients, central nervous system (CNS)-active polypharmacy may increase the risk for impaired cognition, fall-related injury, and death.
Objective: To determine the extent of CNS-active polypharmacy among community-dwelling older adults with dementia in the US.
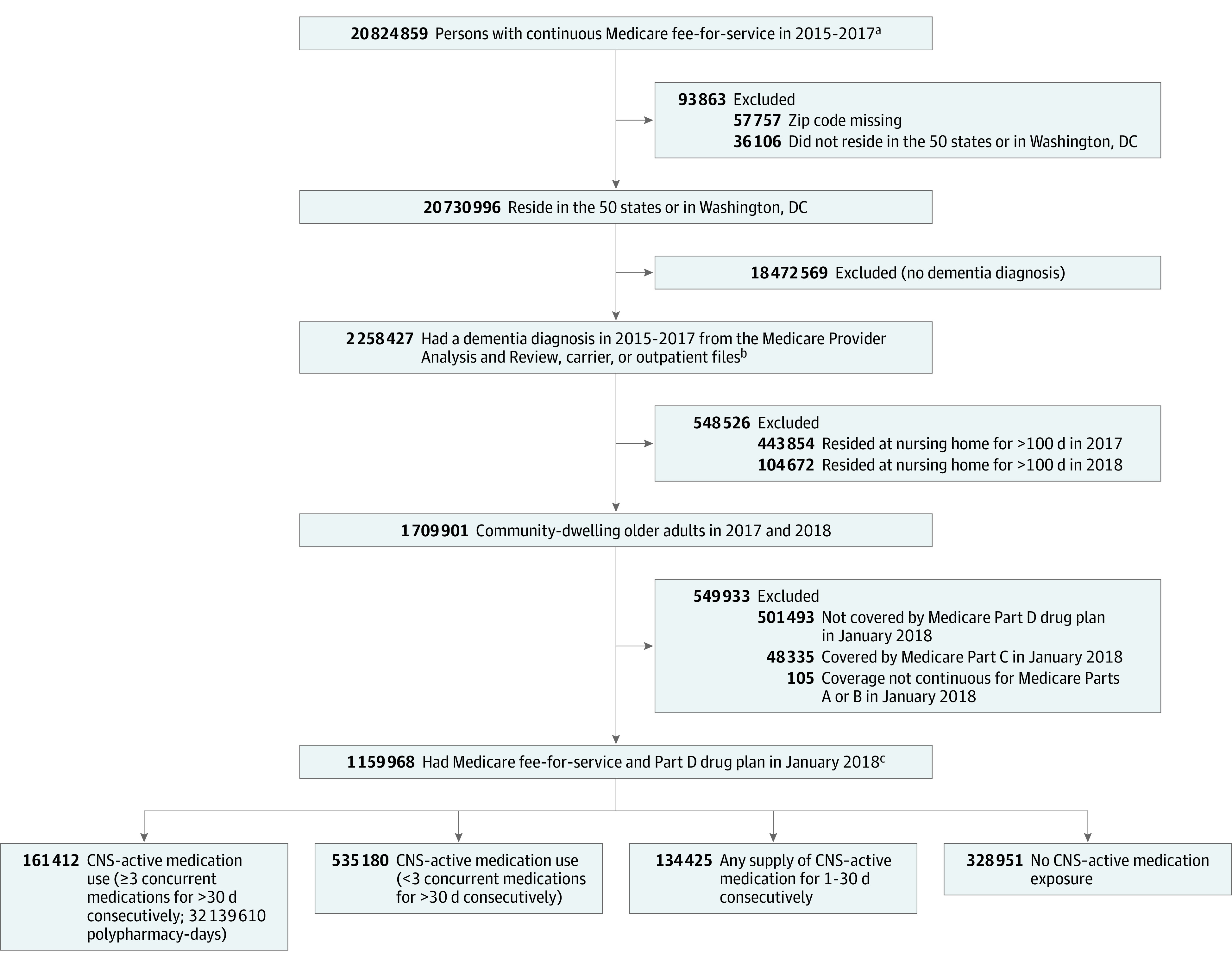
Design, setting, and participants: Cross-sectional analysis of all community-dwelling older adults with dementia (identified by International Classification of Diseases, Ninth Revision, Clinical Modification or International Statistical Classification of Diseases and Related Health Problems, Tenth Revision diagnosis codes; N = 1 159 968) and traditional Medicare coverage from 2015 to 2017. Medication exposure was estimated using prescription fills between October 1, 2017, and December 31, 2018.
Exposures: Part D coverage during the observation year (January 1-December 31, 2018).
Main outcomes and measures: The primary outcome was the prevalence of CNS-active polypharmacy in 2018, defined as exposure to 3 or more medications for longer than 30 days consecutively from the following classes: antidepressants, antipsychotics, antiepileptics, benzodiazepines, nonbenzodiazepine benzodiazepine receptor agonist hypnotics, and opioids. Among those who met the criterion for polypharmacy, duration of exposure, number of distinct medications and classes prescribed, common class combinations, and the most commonly used CNS-active medications also were determined.
Results: The study included 1 159 968 older adults with dementia (median age, 83.0 years [interquartile range {IQR}, 77.0-88.6 years]; 65.2% were female), of whom 13.9% (n = 161 412) met the criterion for CNS-active polypharmacy (32 139 610 polypharmacy-days of exposure). Those with CNS-active polypharmacy had a median age of 79.4 years (IQR, 74.0-85.5 years) and 71.2% were female. Among those who met the criterion for CNS-active polypharmacy, the median number of polypharmacy-days was 193 (IQR, 88-315 polypharmacy-days). Of those with CNS-active polypharmacy, 57.8% were exposed for longer than 180 days and 6.8% for 365 days; 29.4% were exposed to 5 or more medications and 5.2% were exposed to 5 or more medication classes. Ninety-two percent of polypharmacy-days included an antidepressant, 47.1% included an antipsychotic, and 40.7% included a benzodiazepine. The most common medication class combination included an antidepressant, an antiepileptic, and an antipsychotic (12.9% of polypharmacy-days). Gabapentin was the most common medication and was associated with 33.0% of polypharmacy-days.
Conclusions and relevance: In this cross-sectional analysis of Medicare claims data, 13.9% of older adults with dementia in 2018 filled prescriptions consistent with CNS-active polypharmacy. The lack of information on prescribing indications limits judgments about clinical appropriateness of medication combinations for individual patients.
Conflict of interest statement
Figures
Similar articles
-
Clinician contributions to central nervous system-active polypharmacy among older adults with dementia in the United States.J Am Geriatr Soc. 2025 Feb;73(2):422-430. doi: 10.1111/jgs.19256. Epub 2024 Nov 5. J Am Geriatr Soc. 2025. PMID: 39499066 Free PMC article.
-
Secular Trends in Central Nervous System-Active Polypharmacy Among Serial Cross-Sections of US Adults, 2009-2020.Drugs Aging. 2023 Oct;40(10):941-951. doi: 10.1007/s40266-023-01066-w. Epub 2023 Sep 11. Drugs Aging. 2023. PMID: 37695395 Free PMC article.
-
Opioids and Other Central Nervous System-Active Polypharmacy in Older Adults in the United States.J Am Geriatr Soc. 2017 Sep;65(9):2052-2056. doi: 10.1111/jgs.14930. Epub 2017 May 3. J Am Geriatr Soc. 2017. PMID: 28467623 Free PMC article.
-
Using antipsychotic agents in older patients.J Clin Psychiatry. 2004;65 Suppl 2:5-99; discussion 100-102; quiz 103-4. J Clin Psychiatry. 2004. PMID: 14994733 Review.
-
Psychotropic Drug-Associated Pneumonia in Older Adults.Drugs Aging. 2020 Apr;37(4):241-261. doi: 10.1007/s40266-020-00754-1. Drugs Aging. 2020. PMID: 32107741 Free PMC article. Review.
Cited by
-
Brain-Hazardous Medications and Potential Subadequate Antidepressant Dosing in Older Surgical Patients Receiving Home Antidepressants: An Observational Study of a Large US Health System.Anesth Analg. 2024 Jul 1;139(1):155-164. doi: 10.1213/ANE.0000000000006952. Epub 2024 Mar 20. Anesth Analg. 2024. PMID: 38507476 Free PMC article.
-
Association of first anti-seizure medication choice with injuries in older adults with newly diagnosed epilepsy.Seizure. 2023 Jul;109:20-25. doi: 10.1016/j.seizure.2023.05.006. Epub 2023 May 7. Seizure. 2023. PMID: 37178662 Free PMC article.
-
Factors Associated with Potentially Harmful Medication Prescribing in Nursing Homes: A Scoping Review.J Am Med Dir Assoc. 2022 Sep;23(9):1589.e1-1589.e10. doi: 10.1016/j.jamda.2022.06.008. Epub 2022 Jul 20. J Am Med Dir Assoc. 2022. PMID: 35868350 Free PMC article.
-
Comment on "The Relationship Between Antipsychotics, Cognitive Enhancers, and Major Adverse Cardiovascular/Cerebrovascular Events (MACCE) in Older Adults with Behavioral and Psychological Symptoms of Dementia".Drugs Aging. 2024 Oct;41(10):859-861. doi: 10.1007/s40266-024-01152-7. Epub 2024 Oct 9. Drugs Aging. 2024. PMID: 39382801 No abstract available.
-
Central Nervous System Polypharmacy Among People Living With Dementia.J Am Med Dir Assoc. 2025 Aug;26(8):105708. doi: 10.1016/j.jamda.2025.105708. Epub 2025 Jun 14. J Am Med Dir Assoc. 2025. PMID: 40460892 Clinical Trial.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
