

Evaluation of the Benefits and Harms of Lung Cancer Screening With Low-Dose Computed Tomography: Modeling Study for the US Preventive Services Task Force
- PMID: 33687469
- PMCID: PMC9208912
- DOI: 10.1001/jama.2021.1077
Evaluation of the Benefits and Harms of Lung Cancer Screening With Low-Dose Computed Tomography: Modeling Study for the US Preventive Services Task Force
Abstract
Importance: The US Preventive Services Task Force (USPSTF) is updating its 2013 lung cancer screening guidelines, which recommend annual screening for adults aged 55 through 80 years who have a smoking history of at least 30 pack-years and currently smoke or have quit within the past 15 years.
Objective: To inform the USPSTF guidelines by estimating the benefits and harms associated with various low-dose computed tomography (LDCT) screening strategies.
Design, setting, and participants: Comparative simulation modeling with 4 lung cancer natural history models for individuals from the 1950 and 1960 US birth cohorts who were followed up from aged 45 through 90 years.
Exposures: Screening with varying starting ages, stopping ages, and screening frequency. Eligibility criteria based on age, cumulative pack-years, and years since quitting smoking (risk factor-based) or on age and individual lung cancer risk estimation using risk prediction models with varying eligibility thresholds (risk model-based). A total of 1092 LDCT screening strategies were modeled. Full uptake and adherence were assumed for all scenarios.
Main outcomes and measures: Estimated lung cancer deaths averted and life-years gained (benefits) compared with no screening. Estimated lifetime number of LDCT screenings, false-positive results, biopsies, overdiagnosed cases, and radiation-related lung cancer deaths (harms).
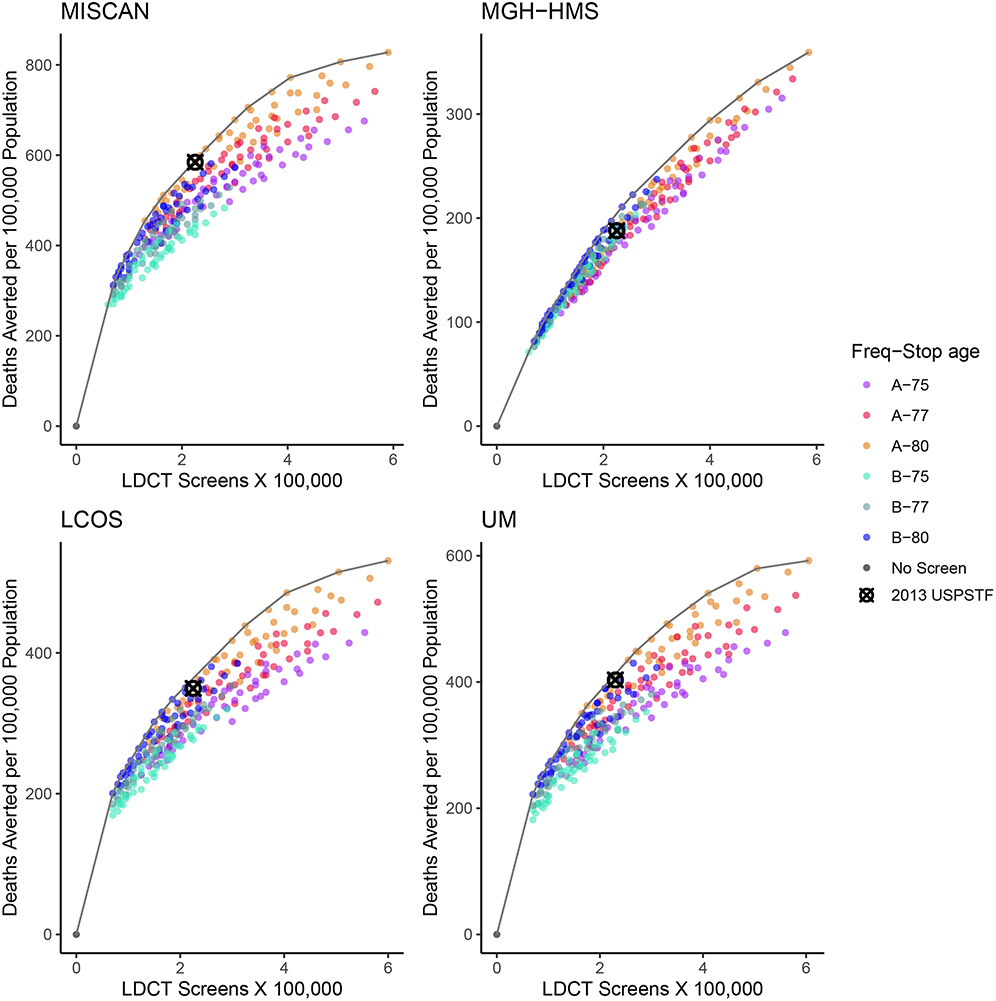
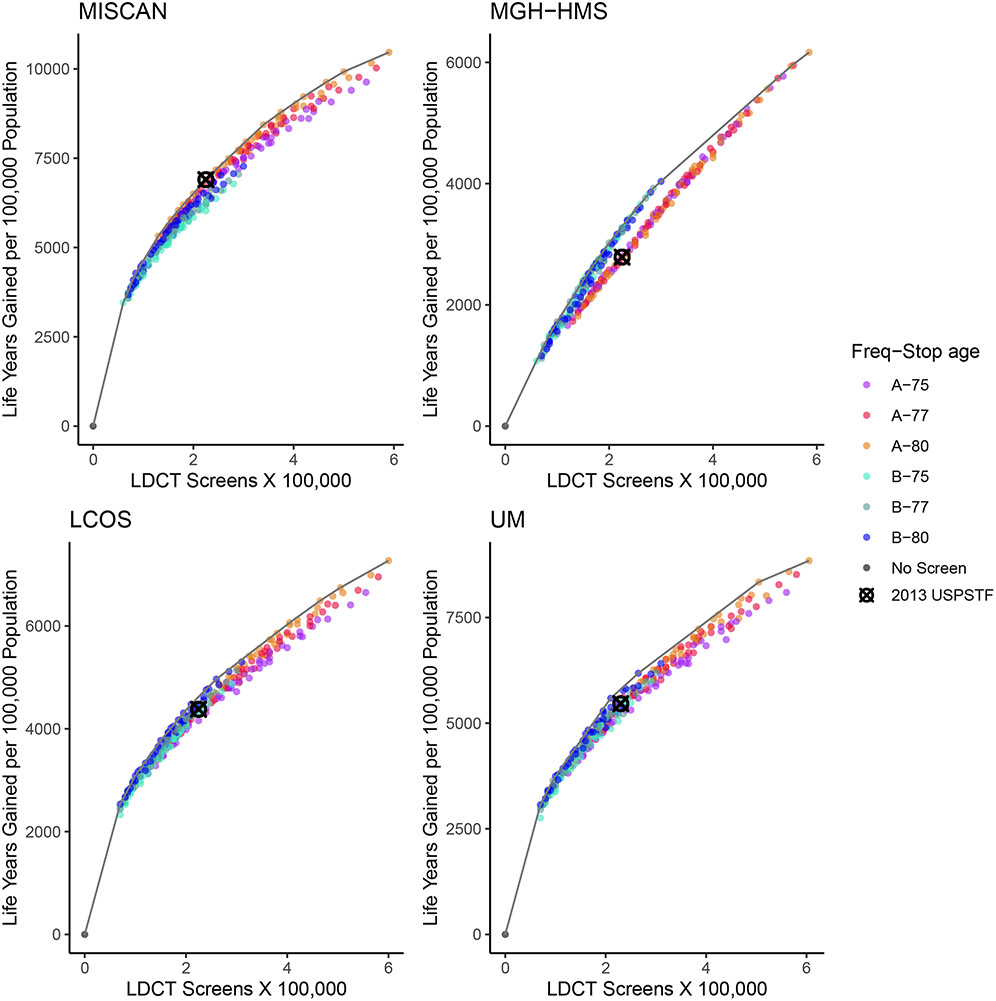
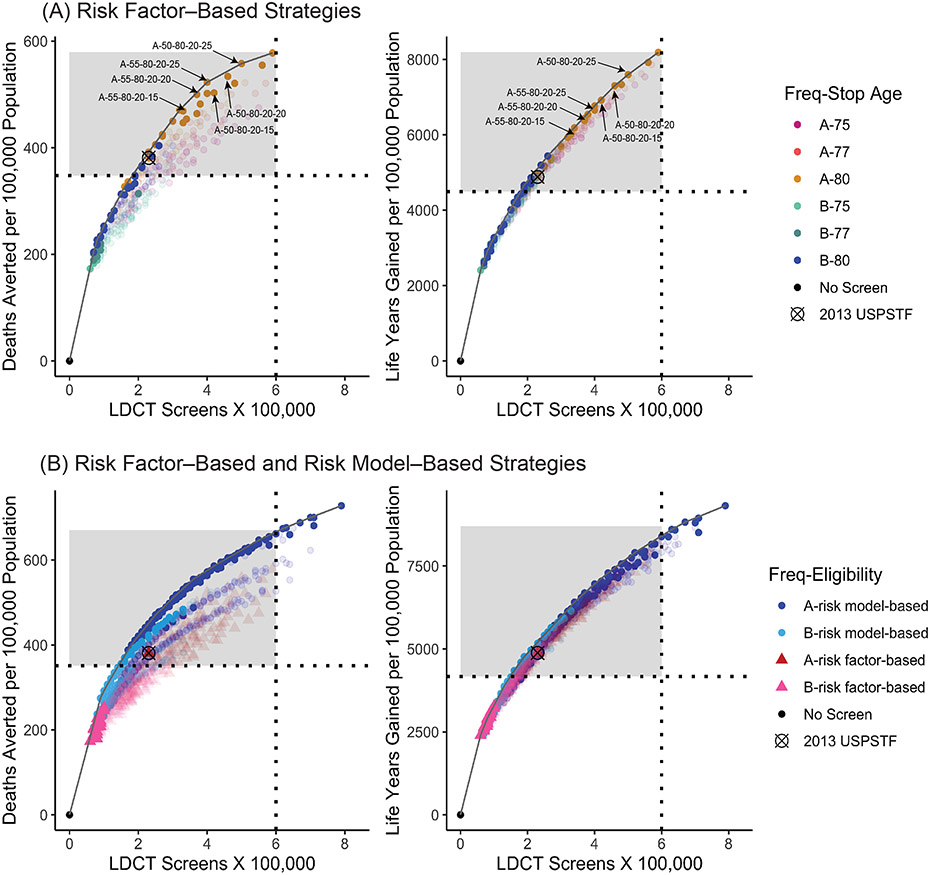
Results: Efficient screening programs estimated to yield the most benefits for a given number of screenings were identified. Most of the efficient risk factor-based strategies started screening at aged 50 or 55 years and stopped at aged 80 years. The 2013 USPSTF-recommended criteria were not among the efficient strategies for the 1960 US birth cohort. Annual strategies with a minimum criterion of 20 pack-years of smoking were efficient and, compared with the 2013 USPSTF-recommended criteria, were estimated to increase screening eligibility (20.6%-23.6% vs 14.1% of the population ever eligible), lung cancer deaths averted (469-558 per 100 000 vs 381 per 100 000), and life-years gained (6018-7596 per 100 000 vs 4882 per 100 000). However, these strategies were estimated to result in more false-positive test results (1.9-2.5 per person screened vs 1.9 per person screened with the USPSTF strategy), overdiagnosed lung cancer cases (83-94 per 100 000 vs 69 per 100 000), and radiation-related lung cancer deaths (29.0-42.5 per 100 000 vs 20.6 per 100 000). Risk model-based vs risk factor-based strategies were estimated to be associated with more benefits and fewer radiation-related deaths but more overdiagnosed cases.
Conclusions and relevance: Microsimulation modeling studies suggested that LDCT screening for lung cancer compared with no screening may increase lung cancer deaths averted and life-years gained when optimally targeted and implemented. Screening individuals at aged 50 or 55 years through aged 80 years with 20 pack-years or more of smoking exposure was estimated to result in more benefits than the 2013 USPSTF-recommended criteria and less disparity in screening eligibility by sex and race/ethnicity.
Conflict of interest statement
Figures
Comment in
-
Expanded Access to Lung Cancer Screening-Implementing Wisely to Optimize Health.JAMA Netw Open. 2021 Mar 1;4(3):e210275. doi: 10.1001/jamanetworkopen.2021.0275. JAMA Netw Open. 2021. PMID: 33687439 No abstract available.
-
Broadened Eligibility for Lung Cancer Screening: Challenges and Uncertainty for Implementation and Equity.JAMA. 2021 Mar 9;325(10):939-941. doi: 10.1001/jama.2020.26422. JAMA. 2021. PMID: 33687453 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
