

Impact of Socioeconomic Status on Presentation and Outcomes in Colorectal Peritoneal Metastases Following Cytoreduction and Chemoperfusion: Persistent Inequalities in Outcomes at a High-Volume Center
- PMID: 33687614
- PMCID: PMC8184539
- DOI: 10.1245/s10434-021-09627-2
Impact of Socioeconomic Status on Presentation and Outcomes in Colorectal Peritoneal Metastases Following Cytoreduction and Chemoperfusion: Persistent Inequalities in Outcomes at a High-Volume Center
Erratum in
-
Correction to: Impact of Socioeconomic Status on Presentation and Outcomes in Colorectal Peritoneal Metastases Following Cytoreduction and Chemoperfusion: Persistent Inequalities in Outcomes at a High-Volume Center.Ann Surg Oncol. 2021 Dec;28(Suppl 3):875. doi: 10.1245/s10434-021-10045-7. Ann Surg Oncol. 2021. PMID: 33893603 Free PMC article. No abstract available.
Abstract
Background: Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion (CRS HIPEC) can offer significant survival advantage for select patients with colorectal peritoneal metastases (CRPM). Low socioeconomic status (SES) is implicated in disparities in access to care. We analyze the impact of SES on postoperative outcomes and survival at a high-volume tertiary CRS HIPEC center.
Patients and methods: We conducted a retrospective cohort study examining patients who underwent CRS HIPEC for CRPM from 2000 to 2018. Patients were grouped according to SES. Baseline characteristics, perioperative outcomes, and survival were examined between groups.
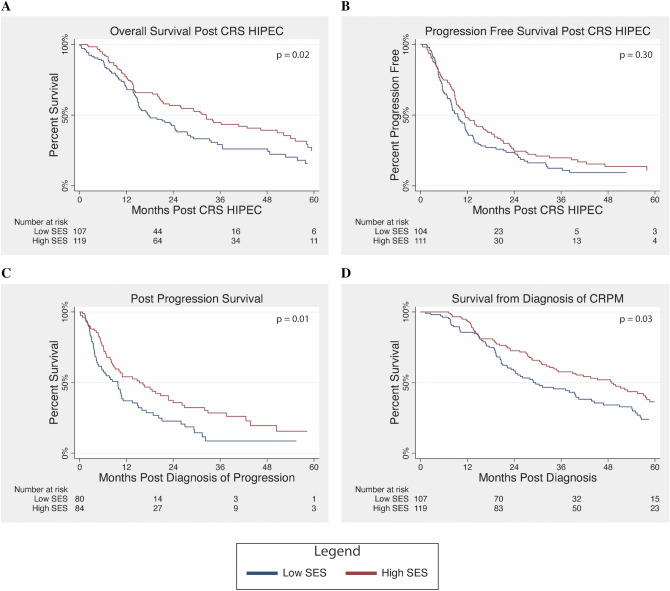
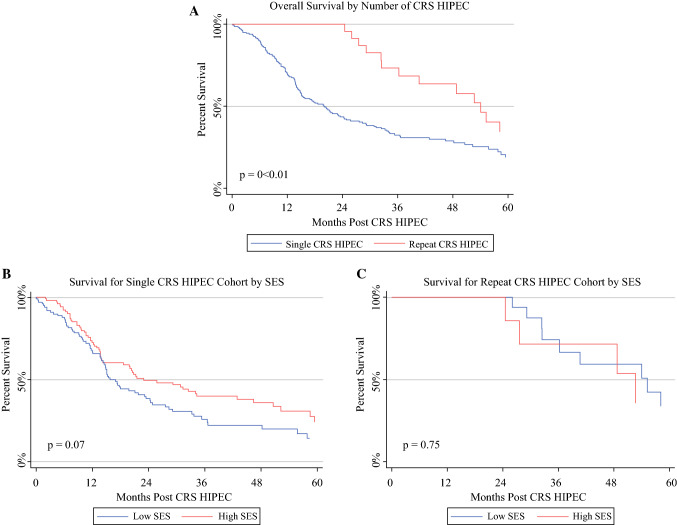
Results: A total of 226 patients were analyzed, 107 (47%) low-SES and 119 (53%) high-SES patients. High-SES patients were younger (52 vs. 58 years, p = 0.01) and more likely to be White (95.0% vs. 91.6%, p = 0.06) and privately insured (83% vs. 57%, p < 0.001). They traveled significantly further for treatment and had lower burden of comorbidities and frailty (p = 0.01). Low-SES patients more often presented with synchronous peritoneal metastases (48% vs. 35%, p = 0.05). Following CRS HIPEC, low-SES patients had longer length of stay and higher burden of postoperative complications, 90-day readmission, and 30-day mortality. Median overall survival following CRS HIPEC was worse for low-SES patients (17.8 vs. 32.4 months, p = 0.02). This disparity persisted on multivariate survival analysis (low SES: HR = 1.46, p = 0.03).
Conclusions: Despite improving therapies for CRPM, low-SES patients remain at a significant disadvantage. Even patients who overcome barriers to care experience worse short- and long-term outcomes. Improving access and addressing these disparities is crucial to ensure equitable outcomes and improve patient care.
Figures
Similar articles
-
Impact of sociodemographic factors on outcomes in patients with peritoneal malignancies following cytoreduction and chemoperfusion.J Surg Oncol. 2022 Jun;125(8):1285-1291. doi: 10.1002/jso.26843. Epub 2022 Mar 6. J Surg Oncol. 2022. PMID: 35253223 Free PMC article.
-
Socioeconomic Barriers to CRS HIPEC for Appendiceal Cancer within a Regional Academic Hospital System.Ann Surg Oncol. 2022 Oct;29(11):6593-6602. doi: 10.1245/s10434-022-11949-8. Epub 2022 May 31. Ann Surg Oncol. 2022. PMID: 35639293 Free PMC article.
-
Impact of Primary Tumor Location and Genomic Alterations on Survival Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemoperfusion for Colorectal Peritoneal Metastases.Ann Surg Oncol. 2023 Jul;30(7):4459-4470. doi: 10.1245/s10434-023-13463-x. Epub 2023 Apr 21. Ann Surg Oncol. 2023. PMID: 37085655 Free PMC article.
-
Repeat Cytoreductive Surgery-Hyperthermic Intraperitoneal Chemoperfusion is Feasible and Offers Survival Benefit in Select Patients with Peritoneal Metastases.Ann Surg Oncol. 2019 May;26(5):1445-1453. doi: 10.1245/s10434-019-07218-w. Epub 2019 Mar 1. Ann Surg Oncol. 2019. PMID: 30825033 Free PMC article.
-
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases - The Hong Kong experience and literature review.Asian J Surg. 2021 Jan;44(1):221-228. doi: 10.1016/j.asjsur.2020.05.010. Epub 2020 Jun 27. Asian J Surg. 2021. PMID: 32605790 Review.
Cited by
-
ASO Author Reflections: Understanding Barriers to Complex Cancer Surgery.Ann Surg Oncol. 2022 Oct;29(11):6603. doi: 10.1245/s10434-022-12014-0. Epub 2022 Jun 21. Ann Surg Oncol. 2022. PMID: 35729290 No abstract available.
-
Impact of sociodemographic factors on outcomes in patients with peritoneal malignancies following cytoreduction and chemoperfusion.J Surg Oncol. 2022 Jun;125(8):1285-1291. doi: 10.1002/jso.26843. Epub 2022 Mar 6. J Surg Oncol. 2022. PMID: 35253223 Free PMC article.
-
Prognostic Factors in Colorectal Liver Metastases: An Exhaustive Review of the Literature and Future Prospectives.Cancers (Basel). 2025 Jul 31;17(15):2539. doi: 10.3390/cancers17152539. Cancers (Basel). 2025. PMID: 40805233 Free PMC article. Review.
-
A call for standardized reporting of early-onset colorectal peritoneal metastases.Eur J Cancer Prev. 2023 Nov 1;32(6):548-556. doi: 10.1097/CEJ.0000000000000816. Epub 2023 Jun 12. Eur J Cancer Prev. 2023. PMID: 37310397 Free PMC article. Review.
-
Socioeconomic Barriers to CRS HIPEC for Appendiceal Cancer within a Regional Academic Hospital System.Ann Surg Oncol. 2022 Oct;29(11):6593-6602. doi: 10.1245/s10434-022-11949-8. Epub 2022 May 31. Ann Surg Oncol. 2022. PMID: 35639293 Free PMC article.
References
-
- Glehen O, Kwiatkowski F, Sugarbaker PH, et al. Cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol. 2004;22(16):3284–3292. doi: 10.1200/jco.2004.10.012. - DOI - PubMed
-
- Verwaal VJ, Bruin S, Boot H, van Slooten G, van Tinteren H. 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol. 2008;15(9):2426–2432. doi: 10.1245/s10434-008-9966-2. - DOI - PubMed
-
- Baratti D, Kusamura S, Iusco D, et al. Postoperative complications after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy affect long-term outcome of patients with peritoneal metastases from colorectal cancer: a two-center study of 101 patients. Dis Colon Rectum. 2014;57(7):858–868. doi: 10.1097/DCR.0000000000000149. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
