

Association of Donor and Recipient Cytomegalovirus Serostatus on Graft and Patient Survival in Liver Transplant Recipients
- PMID: 33687777
- PMCID: PMC9121742
- DOI: 10.1002/lt.26045
Association of Donor and Recipient Cytomegalovirus Serostatus on Graft and Patient Survival in Liver Transplant Recipients
Erratum in
-
Errata.Liver Transpl. 2022 Jul;28(7):1266. doi: 10.1002/lt.26453. Epub 2022 Mar 21. Liver Transpl. 2022. PMID: 35312159 No abstract available.
Abstract
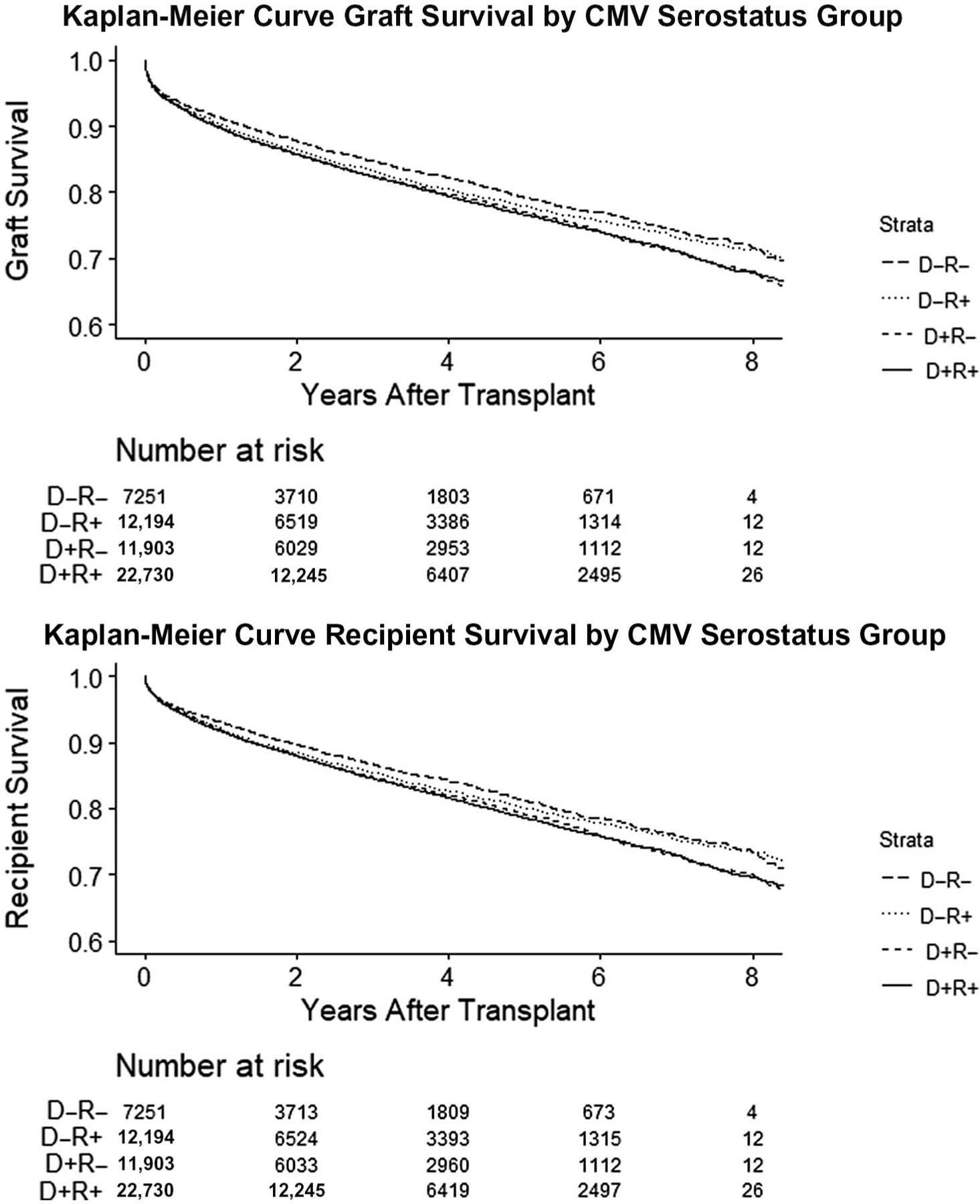
Among solid organ transplant recipients, donor cytomegalovirus (CMV) seropositive (D+) and recipient seronegative (R-) status are associated with an increased risk of graft loss and mortality after kidney or lung transplantation. Whether a similar relationship exists among liver transplant recipients (LTR) is unknown. We assessed graft loss and mortality among adult LTRs from January 1, 2010, to March 14, 2020, in the Organ Procurement and Transplantation Network database. We used multivariable mixed Cox proportional hazards regression to analyze the association of donor and recipient CMV serostatus group with graft loss and mortality, with donor seronegative (D-) and recipient seronegative (R-) as the reference group. Among 54,078 LTRs, the proportion of D-R-, D- and recipient seropositive (R+), D+R-, and D+R+ was 13.4%, 22.5%, 22%, and 42%, respectively. By unadjusted Kaplan-Meier survival curve estimates, survival by the end of follow-up was 73.3%, 73.5%, 70.1%, and 69.7%, among the D-R-, D-R+, D+R-, and D+R+ groups, respectively. By multivariable Cox regression, the CMV D+R- serogroup, but not other serogroups, was independently associated with increased risks of graft loss (adjusted hazard ratio [aHR], 1.13; 95% confidence interval [CI], 1.05-1.22) and mortality (aHR, 1.13; 95% CI, 1.05-1.22). The magnitude of the association of the CMV D+R- serostatus group with mortality was similar when the Cox regression analysis was restricted to the first year after transplant and beyond the first year after transplant: aHR, 1.13 (95% CI, 1.01-1.27) and aHR, 1.13 (95% CI, 1.02-1.25), respectively. Even in an era of CMV preventive strategies, CMV D+R- serogroup status remains independently associated with increased graft loss and mortality in adult LTRs. Factors in addition to direct CMV-associated short-term mortality are likely, and studies to define the underlying mechanism(s) are warranted.
Copyright © 2021 by the American Association for the Study of Liver Diseases.
Figures
References
-
- Bosch W, Heckman MG, Diehl NN, Shalev JA, Pungpapong S, Hellinger WC. Association of cytomegalovirus infection and disease with death and graft loss after liver transplant in high-risk recipients. Am J Transplant 2011;11:2181–2189. - PubMed
-
- Limaye AP, Bakthavatsalam R, Kim HW, Randolph SE, Halldorson JB, Healey PJ, et al. Impact of cytomegalovirus in organ transplant recipients in the era of antiviral prophylaxis. Transplantation 2006;81:1645–1652. - PubMed
-
- Razonable RR, Humar A. Cytomegalovirus in solid organ transplant recipients—guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant 2019;33:e13512. - PubMed
-
- Katsolis JG, Bosch W, Heckman MG, Diehl NN, Shalev JA, Pungpapong S, et al. Evaluation of risk factors for cytomegalovirus infection and disease occurring within 1 year of liver transplantation in high-risk patients. Transpl Infect Dis 2013;15:171–180. - PubMed
-
- Limaye AP, Bakthavatsalam R, Kim HW, Kuhr CS, Halldorson JB, Healey PJ, et al. Late-onset cytomegalovirus disease in liver transplant recipients despite antiviral prophylaxis. Transplantation 2004;78:1390–1396. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
