

Antithrombotic therapy to prevent recurrent pregnancy loss in antiphospholipid syndrome-What is the evidence?
- PMID: 33687789
- PMCID: PMC8252114
- DOI: 10.1111/jth.15290
Antithrombotic therapy to prevent recurrent pregnancy loss in antiphospholipid syndrome-What is the evidence?
Abstract
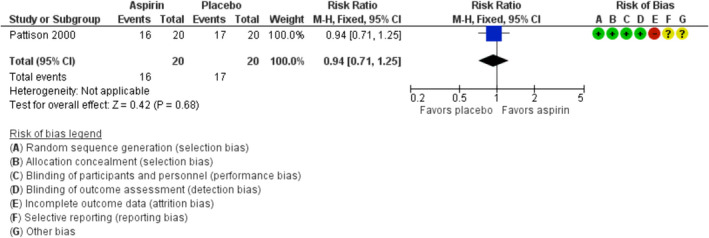
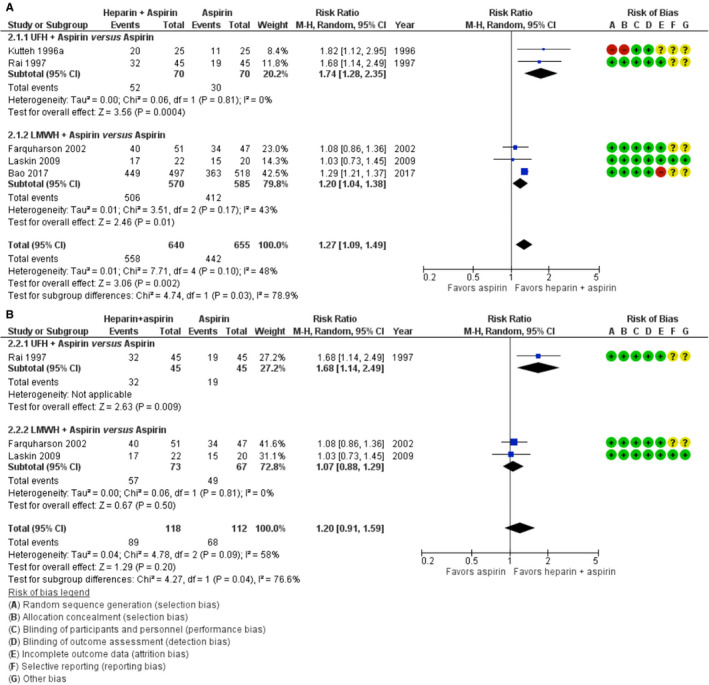
Aspirin and heparin are widely used to reduce the risk of recurrent pregnancy loss in women with antiphospholipid syndrome. This practice is based on only a few intervention studies, and uncertainty regarding benefits and risk remains. In this case-based review, we summarize the available evidence and address the questions that are most important for clinical practice. We performed a systematic review of randomized controlled trials assessing the effect of heparin (low molecular weight heparin [LMWH] or unfractionated heparin [UFH]), aspirin, or both on live birth rates in women with persistent antiphospholipid antibodies and recurrent pregnancy loss. Eleven trials including 1672 women met the inclusion criteria. Aspirin only did not increase live birth rate compared to placebo in one trial of 40 women (risk ratio [RR] 0.94; 95% confidence interval [CI] 0.71-1.25). One trial of 141 women reported a higher live birth rate with LMWH only than with aspirin only (RR 1.20; 95% CI 1.00-1.43). Five trials totaling 1295 women compared heparin plus aspirin with aspirin only. The pooled RR for live birth was 1.27 (95% CI 1.09-1.49) in favor of heparin plus aspirin. There was significant heterogeneity between the subgroups of LMWH and UFH (RR for LWMH plus aspirin versus aspirin 1.20, 95% CI: 1.04-1.38; RR for UFH plus aspirin versus aspirin 1.74, 95% CI: 1.28-2.35; I2 78.9%, p = .03). Characteristics of participants and adverse events were not uniformly reported. Heparin (LMWH or UFH) plus aspirin may improve live birth rates in women with recurrent pregnancy loss and antiphospholipid antibodies, but evidence is of low certainty.
Keywords: antiphospholipid syndrome; heparin; live birth; recurrent pregnancy loss-aspirin.
© 2021 The Authors. Journal of Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis.
Conflict of interest statement
S. Middeldorp reports grants and fees paid to her institution from GSK, BMS/Pfizer, Aspen, Daiichi Sankyo, Bayer, Boehringer Ingelheim, Sanofi, and Portola. L.J.J. Scheres received funding for the printing of his doctoral thesis from the Dutch Heart Foundation, Dutch Federation of Coagulation Clinics, Stichting tot Steun Promovendi Vasculaire Geneeskunde, Bayer, Daiichi Sankyo, LEO Pharma, and Pfizer, outside the submitted work. M. Goddijn works at the Department of Reproductive Medicine of the Amsterdam UMC (location AMC and location VUmc). Location VUMC has received several research and educational grants from Guerbet, Merck, and Ferring, not related to the presented work. E.N. Hamulyák has nothing to disclose.
Figures
References
-
- Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO. VTE, Thrombophilia, Antithrombotic Therapy, and Pregnancy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2):e691S‐e736S. - PMC - PubMed
-
- Committee on Practice Bulletins—Obstetrics, American College of Obstetricians and Gynecologists . Practice Bulletin No. 132: Antiphospholipid syndrome. Obstet Gynecol. 2012;120(6):1514‐1521. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
