

Radiation-Associated Lymphopenia and Outcomes of Patients with Unresectable Hepatocellular Carcinoma Treated with Radiotherapy
- PMID: 33688489
- PMCID: PMC7937383
- DOI: 10.2147/JHC.S282062
Radiation-Associated Lymphopenia and Outcomes of Patients with Unresectable Hepatocellular Carcinoma Treated with Radiotherapy
Abstract
Background: The immune system plays a crucial role in cancer surveillance. Previous studies have shown that lymphopenia associated with radiotherapy (RT) portends a poor prognosis. We sought to differentiate the effects of proton and photon RT on changes in absolute lymphocyte count (ALC) for patients with hepatocellular carcinoma (HCC).
Patients and methods: Patients with HCC treated with definitive RT from 2006 to 2016 were studied. Serial ALCs were graded according to CTCAE v4.0. Overall survival (OS), disease-free survival, and distant metastasis-free survival were analyzed using the Kaplan-Meier method. Univariable and multivariable Cox-proportional hazards analyses were used to identify predictors of OS. A cohort analysis matched for treatment volume was performed to investigate differences in ALC dynamics between photon and proton therapy.
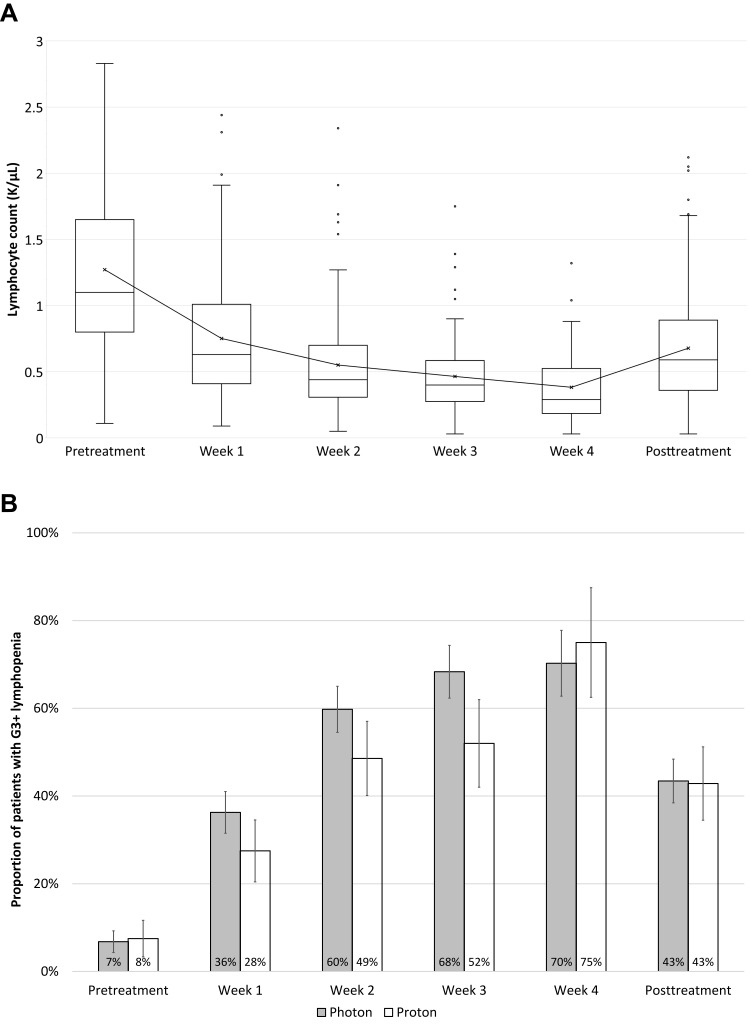
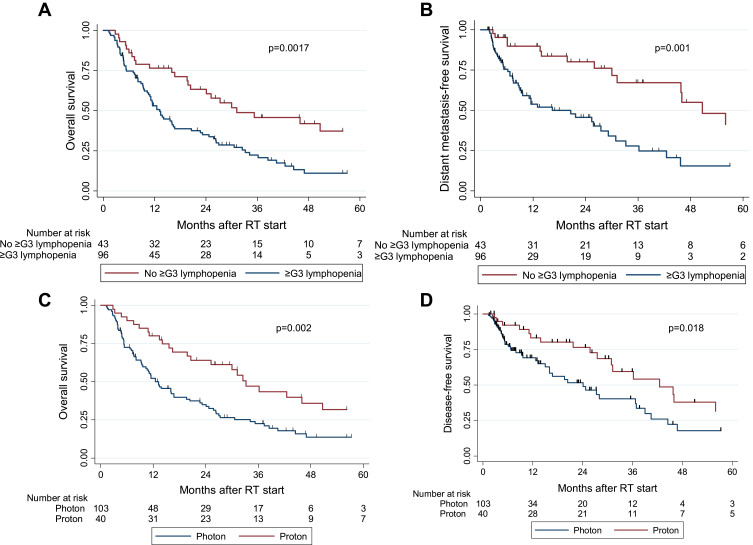
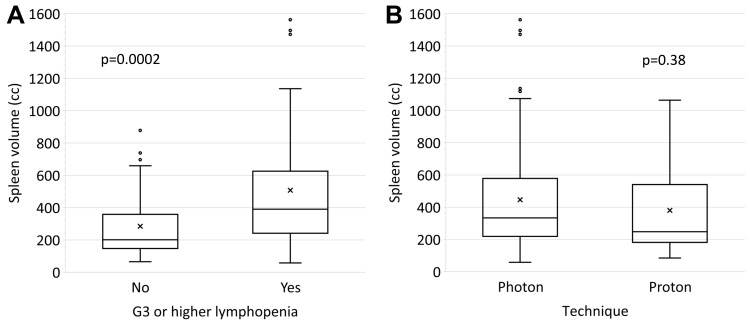
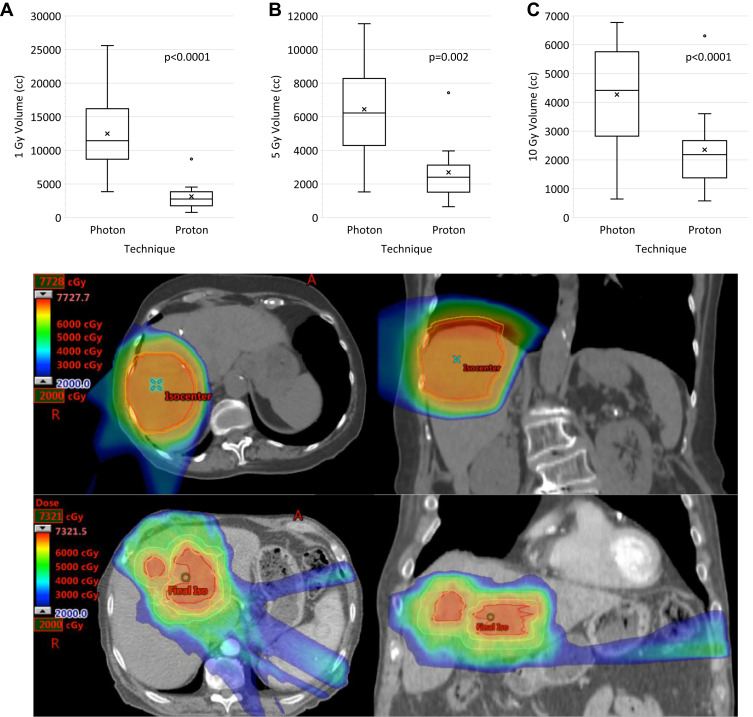
Results: Of 143 patients identified, the median age was 66 (range, 19-90) years. The treatment modality was photon in 103 (72%) and proton in 40 (28%). Median follow-up was 17 months (95% confidence interval, 13-25 months). The median time to ALC nadir after initiation of RT was 17 days with a median relative decrease of 67%. Those who received proton RT had a higher median ALC nadir (0.41 vs 0.32 k/µL, p=0.002) and longer median OS (33 vs 13 months, p=0.002) than those who received photon RT. Matched cohort analyses revealed a larger low-dose liver volume in the photon group, which correlated with lower ALC. On multivariable Cox analysis, Grade 3 or higher lymphopenia prior to or after RT, portal venous tumor thrombus, larger planning target volumes, Child-Pugh (CP) Class B, and increased CP score after RT were associated with a higher risk of death, whereas the use of proton therapy was associated with lower risk.
Conclusion: Grade 3 or higher lymphopenia may be associated with poorer outcomes in patients receiving RT for HCC. Protons may mitigate lymphopenia compared with photons, potentially due to reduced dose exposure of sites of lymphopoiesis.
Keywords: circulating lymphocytes; liver dose; lymphocyte count; overall survival; splenic dose.
© 2021 De et al.
Conflict of interest statement
BD reports honorarium from Sermo, Inc. ACK reports ownership of shares in Aravive, Inc. SPN reports funding from the Australian Postgraduate Award, the Royal Australian and New Zealand College of Radiologists (RANZCR) Research Grants, and the Radiological Society of North America (RSNA) Fellow Grant. JMH reports research support from Oncosil, Galera, Auro, and Augmenix and is also a consultant for BTG, AbbVie, Celgene, AstraZeneca, BMS, and Varian. RT reports personal fees from QED Therapeutics/The Lynx Group. EBH reports grants from Merck. SK reports grants from NIH, DoD, and CPRIT. In addition, SK reports a patent for minibeam therapy. TSH reports consulting fees from Merck, Novocure, Synthetic Biologics, and research funding from Taiho, Astra-Zeneca, BMS, Puma, IntraOp, and Tesaro. SHL reports grants and personal fees from Beyond Spring Pharmaceuticals and Hitachi Chemical Diagnostics, as well as personal fees from AstraZeneca, Inc and STCube Pharmaceuticals. EJK reports grants from National Institutes of Health, Stand Up 2 Cancer, MD Anderson Cancer Center, Elekta, and GE Healthcare, as well as personal fees from RenovoRx and Taylor and Francis. All reported conflicts are outside the submitted work. The authors report no other conflicts of interest in this work.
Figures
References
-
- SEER. Cancer stat facts: liver and intrahepatic bile duct cancer. Available from: https://seer.cancer.gov/statfacts/html/livibd.html. Accessed November21, 2020.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
