

Outcome trends in people with heart failure, type 2 diabetes mellitus and chronic kidney disease in the UK over twenty years
- PMID: 33688855
- PMCID: PMC7910705
- DOI: 10.1016/j.eclinm.2021.100739
Outcome trends in people with heart failure, type 2 diabetes mellitus and chronic kidney disease in the UK over twenty years
Abstract
Background: Heart failure (HF) together with type 2 diabetes (T2D) and chronic kidney disease (CKD) are major pandemics of the twenty first century. It is not known in people with new onset HF, what the distinct and combined associations are between T2D and CKD comorbidities and cause-specific hospital admissions and death, over the past 20 years.
Methods: An observational study using the UK Clinical Practice Research Datalink linked to the Hospital Episode Statistics in England (1998-2017). Participants were people aged ≥30 years with new onset HF. Exposure groups were HF with: (i) no T2D and no CKD (reference group); (ii) CKD-only (estimated glomerular filtration rate (eGFR) <60 ml/min per 1.73 m2); (iii) T2D-only; (iv) T2D and CKD. CKD severity groups were: CKD-3a (eGFR 45-59); CKD-3b (30-44); CKD-4 (15-29); CKD-5 (<15). Outcomes were cardiovascular and non-cardiovascular hospitalisations and all-cause death.
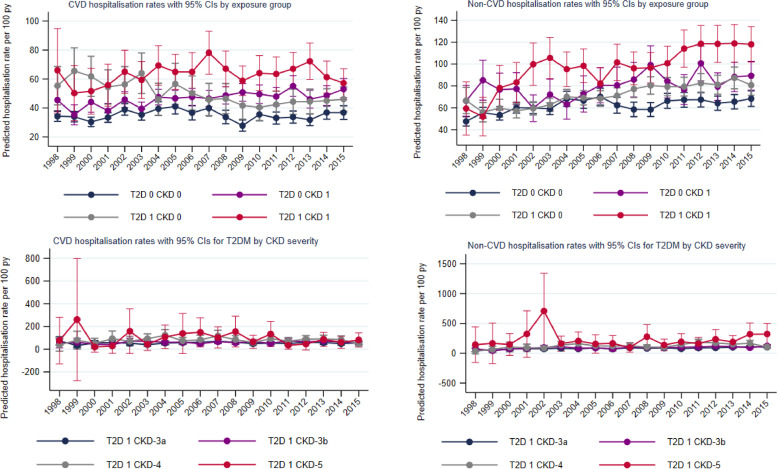
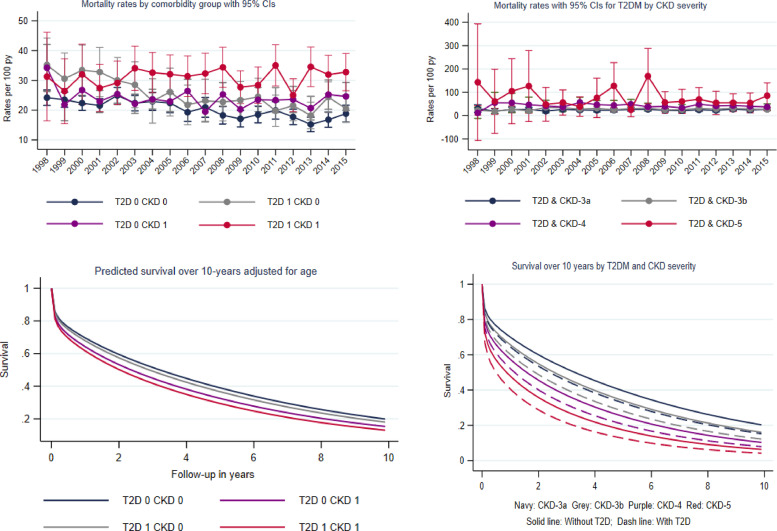
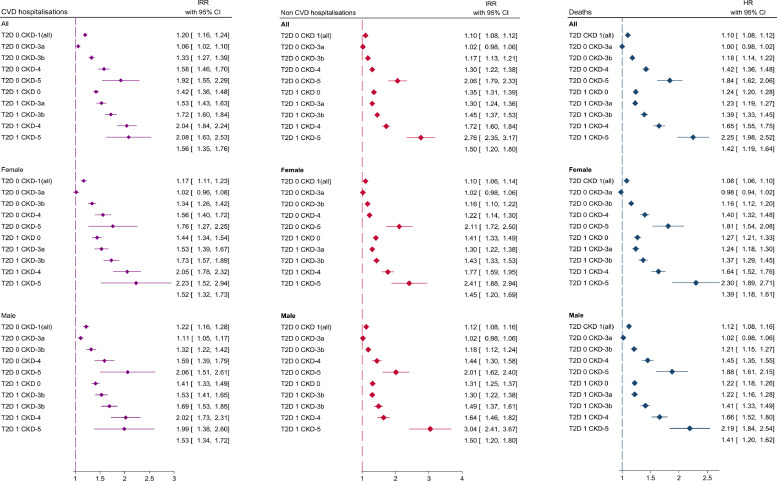
Findings: In 87,709 HF patients (mean age, 78 years; 49% female), 40% had CKD-only, 12% T2D-only, and 16% both. Age-standardised first-year CVD hospitalisation rates were significantly higher in HF patients with CKD-only (46.4; 95% CI 44.9,47.9 per 100 person years) and T2D-only (49.2; 46.7,58.8) than in the reference group (35.1; 34.0,36.1); the highest rate was in patients with T2D-CKD-5: 89.1 (65.8,112.4). Similar patterns were observed for non-CVD hospitalisations and deaths. Group differences remained significant after adjustment for potential confounders. Median survival was highest in the reference (4.4 years) and HF-T2D-only (4.1 years) groups, compared to HF-CKD-only (2.2 years). HF-T2D-CKD group survival ranged from 2.8 (CKD-3a) to 0.7 years (CKD-5). Over time, CVD hospitalisation rates significantly increased for HF-CKD-only (+26%) and reduced (-24%) for HF-T2D-only groups; no reductions were observed in any of the HF-T2D-CKD groups. Trends were similar for non-CVD hospitalisations and death: whilst death rates significantly reduced for HF-T2D-only (-37%), improvement was not observed in any of the T2D-CKD groups.
Interpretation: In a cohort of people with new onset HF, hospitalisations and deaths are high in patients with T2D or CKD, and worst in those with both comorbidities. Whilst outcomes have improved over time for patients with HF and comorbid T2D, similar trends were not seen in those with comorbid CKD. Strategies to prevent and manage CKD in people with HF are urgently needed.
Funding: NIHR fellowship [reference: NIHR 30011].
Keywords: Cardiovascular; Chronic kidney disease; Heart failure; Hospitalisation; Mortality; Type 2 diabetes.
© 2021 The Author(s).
Conflict of interest statement
Dr. Khunti reports personal fees from Amgen, personal fees from Astrazeneca, personal fees from Bayer, personal fees from NAPP, personal fees from Lilly, personal fees from Merck Sharp & Dohme, personal fees from Novartis, personal fees from Novo Nordisk, personal fees from Roche, personal fees from Berlin-Chemie AG / Menarini Group, personal fees from Sanofi-Aventis, personal fees from Servier, personal fees from Boehringer Ingelheim, grants from Pfizer, grants from Boehringer Ingelheim, grants from AstraZeneca, grants from Novartis, grants from Novo Nordisk, grants from Sanofi-Aventis, grants from Lilly, grants from Merck Sharp & Dohme, grants from Servier, outside the submitted work; . Dr. Seidu reports personal fees from Amgen, personal fees from Astrazeneca, personal fees from NAPP, personal fees from Lilly, personal fees from Merck Sharp & Dohme, personal fees from Novartis, personal fees from Novo Nordisk, personal fees from Roche, personal fees from Sanofi-Aventis, personal fees from Boehringer Ingelheim, grants from AstraZeneca, grants from Sanofi-Aventis, grants from Servier, grants from Janssen, outside the submitted work; Dr. Heerspink reports other from Consultant to Abbvie, AstraZeneca, Bayer, Boehringer Ingelheim, Chinook, CSL-Pharma, Janssen, Gilead, MundiPharma, Mitsubishi Tanabe, Merck and Retrophin, grants from Research Grants from Abbvie, AstraZeneca, Boehringer Ingelheim and Janssen, outside the submitted work; . Professor Davies reports personal fees from Novo Nordisk, Sanofi-Aventis, Lilly, Merck Sharp & Dohme, Boehringer Ingelheim, AstraZeneca and Janssen, personal fees from Servier and Gilead Sciences Ltd, personal fees from NAPP, Mitsubishi Tanabe Pharma Corporation and Takeda Pharmaceuticals International Inc., grants from Novo Nordisk, Sanofi-Aventis, Lilly, Boehringer Ingelheim, Astrazeneca and Janssen, outside the submitted work; . Dr. Gerry McCann reports and Research grants from the BHF and NIHR related to T2D and Heart failure. Carolyn SP Lam is supported by a Clinician Scientist Award from the National Medical Research Council of Singapore; has received research support from Boston Scientific, Bayer, Roche Diagnostics, AstraZeneca, Medtronic and Vifor Pharma; has served as consultant or on the Advisory Board/ Steering Committee/ Executive Committee for Boston Scientific, Bayer, Roche, Diagnostics, AstraZeneca, Medtronic, Vifor Pharma, Novartis, Amgen, Merck, Janssen Research & Development LLC, Menarini, Boehringer Ingelheim, Novo Nordisk, Abbott Diagnostics, Corvia, Stealth BioTherapeutics, JanaCare, Biofourmis, Darma, Applied Therapeutics, MyoKardia, Cytokinetics, WebMD Global LLC, Radcliffe Group Lted and Corpis; and serves as co-founder & non-executive director of eKo.ai All the other authors have nothing to disclose.
Figures
References
-
- Mozaffarian D. Executive summary: heart disease and stroke statistics—2015 update: a report from the American heart association. Circulation. 2015;131(4):434–441. - PubMed
-
- Deedwania P., Acharya T. Cardiovascular protection with anti-hyperglycemic agents. Am J Cardiovasc Drugs. 2019;19(3):249–257. - PubMed
-
- Dowrick C. Sage Publications Sage UK; London, England: 2005. What is chronic illness?
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
