

Use of Machine Learning Models to Predict Death After Acute Myocardial Infarction
- PMID: 33688915
- PMCID: PMC7948114
- DOI: 10.1001/jamacardio.2021.0122
Use of Machine Learning Models to Predict Death After Acute Myocardial Infarction
Abstract
Importance: Accurate prediction of adverse outcomes after acute myocardial infarction (AMI) can guide the triage of care services and shared decision-making, and novel methods hold promise for using existing data to generate additional insights.
Objective: To evaluate whether contemporary machine learning methods can facilitate risk prediction by including a larger number of variables and identifying complex relationships between predictors and outcomes.
Design, setting, and participants: This cohort study used the American College of Cardiology Chest Pain-MI Registry to identify all AMI hospitalizations between January 1, 2011, and December 31, 2016. Data analysis was performed from February 1, 2018, to October 22, 2020.
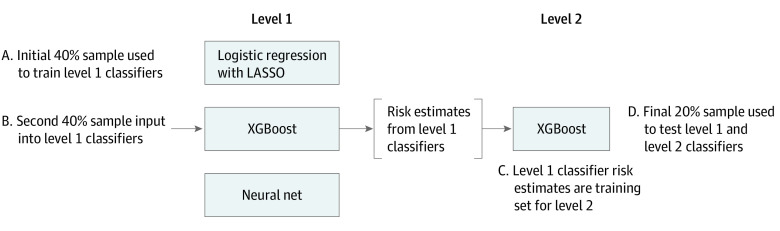
Main outcomes and measures: Three machine learning models were developed and validated to predict in-hospital mortality based on patient comorbidities, medical history, presentation characteristics, and initial laboratory values. Models were developed based on extreme gradient descent boosting (XGBoost, an interpretable model), a neural network, and a meta-classifier model. Their accuracy was compared against the current standard developed using a logistic regression model in a validation sample.
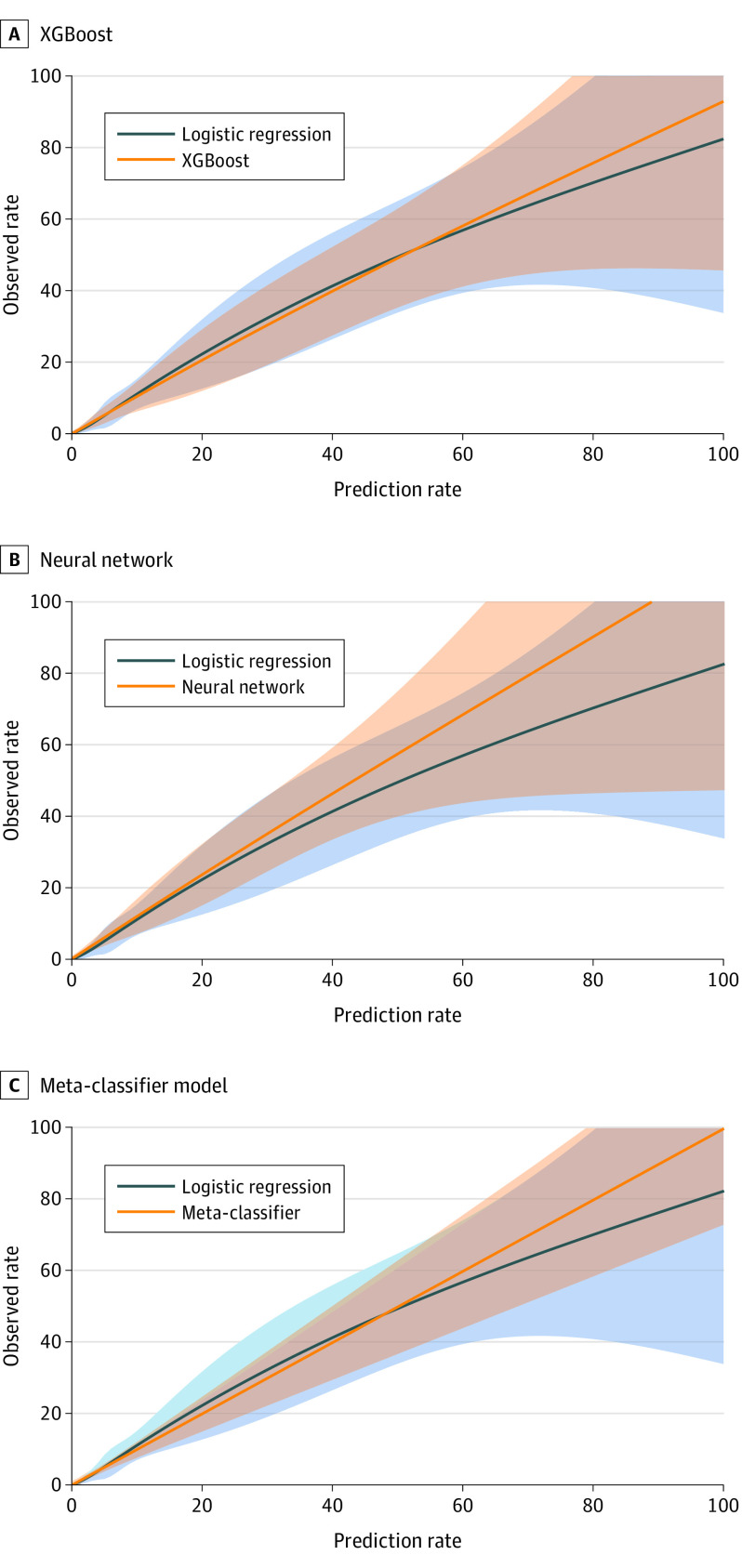
Results: A total of 755 402 patients (mean [SD] age, 65 [13] years; 495 202 [65.5%] male) were identified during the study period. In independent validation, 2 machine learning models, gradient descent boosting and meta-classifier (combination including inputs from gradient descent boosting and a neural network), marginally improved discrimination compared with logistic regression (C statistic, 0.90 for best performing machine learning model vs 0.89 for logistic regression). Nearly perfect calibration in independent validation data was found in the XGBoost (slope of predicted to observed events, 1.01; 95% CI, 0.99-1.04) and the meta-classifier model (slope of predicted-to-observed events, 1.01; 95% CI, 0.99-1.02), with more precise classification across the risk spectrum. The XGBoost model reclassified 32 393 of 121 839 individuals (27%) and the meta-classifier model reclassified 30 836 of 121 839 individuals (25%) deemed at moderate to high risk for death in logistic regression as low risk, which were more consistent with the observed event rates.
Conclusions and relevance: In this cohort study using a large national registry, none of the tested machine learning models were associated with substantive improvement in the discrimination of in-hospital mortality after AMI, limiting their clinical utility. However, compared with logistic regression, XGBoost and meta-classifier models, but not the neural network, offered improved resolution of risk for high-risk individuals.
Conflict of interest statement
Figures
Comment in
-
Incremental Benefits of Machine Learning-When Do We Need a Better Mousetrap?JAMA Cardiol. 2021 Jun 1;6(6):621-623. doi: 10.1001/jamacardio.2021.0139. JAMA Cardiol. 2021. PMID: 33688913 No abstract available.
-
Assessing Performance of Machine Learning.JAMA Cardiol. 2021 Dec 1;6(12):1465. doi: 10.1001/jamacardio.2021.3712. JAMA Cardiol. 2021. PMID: 34586335 No abstract available.
References
-
- Souza AD, Migon HS. Bayesian binary regression model: an application to in-hospital death after AMI prediction. Pesquisa Operacional. 2004;24(2):253-267. doi: 10.1590/S0101-74382004000200003 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
