

Routine versus selective intraoperative cholangiography during cholecystectomy: systematic review, meta-analysis and health economic model analysis of iatrogenic bile duct injury
- PMID: 33688957
- PMCID: PMC7944855
- DOI: 10.1093/bjsopen/zraa032
Routine versus selective intraoperative cholangiography during cholecystectomy: systematic review, meta-analysis and health economic model analysis of iatrogenic bile duct injury
Abstract
Background: Bile duct injury (BDI) is a severe complication following cholecystectomy. Early recognition and treatment of BDI has been shown to reduce costs and improve patients' quality of life. The aim of this study was to assess the effect and cost-effectiveness of routine versus selective intraoperative cholangiography (IOC) in cholecystectomy.
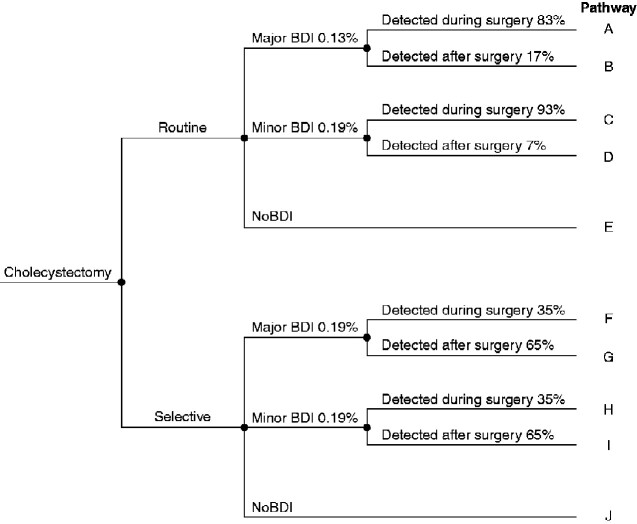
Methods: A systematic review and meta-analysis, combined with a health economic model analysis in the Swedish setting, was performed. Costs per quality-adjusted life-year (QALY) for routine versus selective IOC during cholecystectomy for different scenarios were calculated.
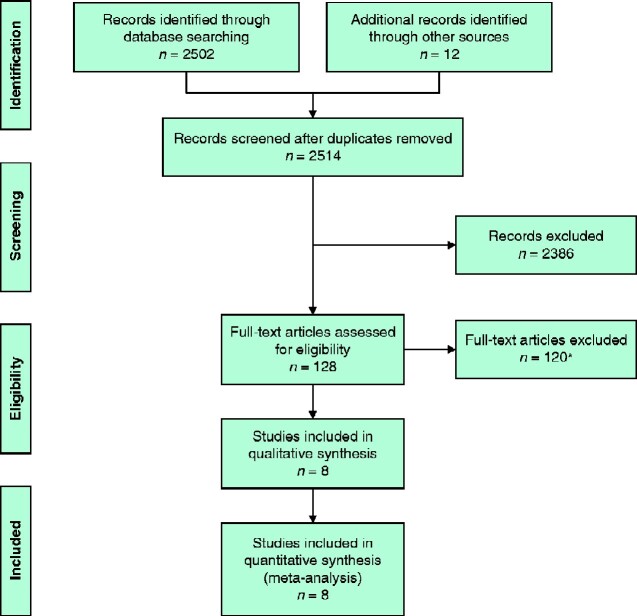
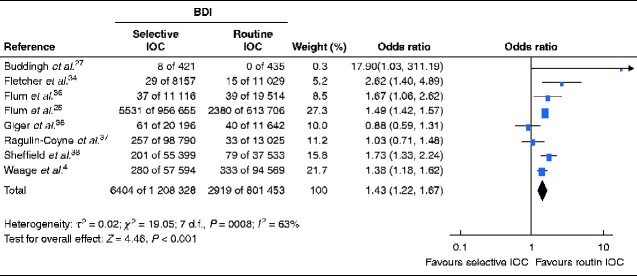
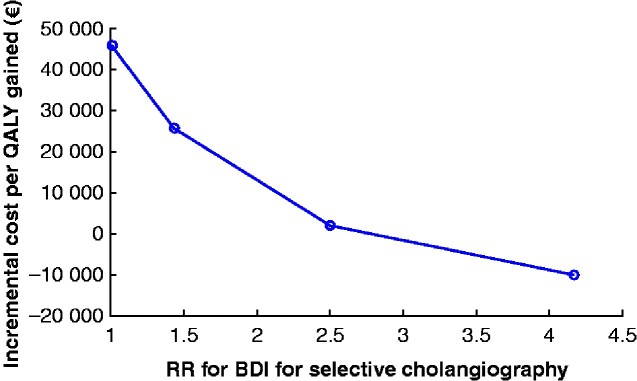
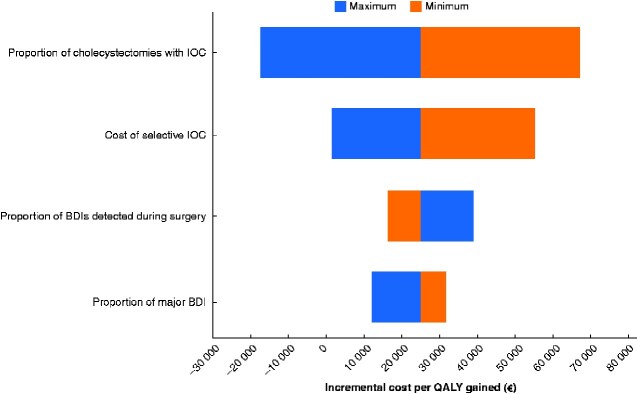
Results: In this meta-analysis, eight studies with more than 2 million patients subjected to cholecystectomy and 9000 BDIs were included. The rate of BDI was estimated to 0.36 per cent when IOC was performed routinely, compared with to 0.53 per cent when used selectively, indicating an increased risk for BDI of 43 per cent when IOC was used selectively (odds ratio 1.43, 95 per cent c.i. 1.22 to 1.67). The model analysis estimated that seven injuries were avoided annually by routine IOC in Sweden, a population of 10 million. Over a 10-year period, 33 QALYs would be gained at an approximate net cost of €808 000 , at a cost per QALY of about €24 900.
Conclusion: Routine IOC during cholecystectomy reduces the risk of BDI compared with the selective strategy and is a potentially cost-effective intervention.
Antecedentes: La lesión de la vía biliar (bile duct injury, BDI) es una complicación grave de la colecistectomía. Se ha demostrado que la detección y el tratamiento precoz de la BDI reducen los costes y mejoran la calidad de vida del paciente (quality-of-life, QoL). El objetivo del estudio fue evaluar el efecto y el coste-beneficio de la colangiografía intraoperatoria (intraoperative cholangiography, IOC) de rutina versus la IOC selectiva durante la colecistectomía.
Métodos: Se realizó una revisión sistemática y un metaanálisis combinados con un análisis del modelo económico de salud en el entorno sueco. Se calculó el coste por año de vida ajustado por calidad (quality-adjusted life-year, QALY) para la IOC de rutina versus la IOC selectiva durante la colecistectomía para diferentes escenarios.
Resultados: En este metaanálisis se incluyeron ocho estudios con más de 2 millones de pacientes sometidos a colecistectomía y 9.000 BDIs. La tasa de BDI se estimó en un 0,36% cuando la IOC se realizó de forma rutinaria, en comparación con un 0,53% cuando se utilizó de forma selectiva, lo que implicaba un aumento del riesgo de BDI del 43% cuando se utilizó la IOC de forma selectiva (razón de oportunidades, odds ratio, OR 1,43; i.c. del 95% 1,22 a 1,67). El análisis del modelo económico estimó que la IOC de rutina evitaba siete lesiones al año en Suecia, una población de 10 millones de personas. Durante un periodo de diez años, se obtendrían 33 QALYs a un coste neto de 808.000 € con un coste por QALY de 24.900 €.
Conclusión: La IOC de rutina durante la colecistectomía reduce el riesgo de BDI en comparación con la estrategia de la realización selectiva y es una intervención potencialmente rentable.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Comment on: Routine versus selective intraoperative cholangiography during cholecystectomy: systematic review, meta-analysis, and health economic model analysis of iatrogenic bile duct injury.BJS Open. 2022 Mar 8;6(2):zrac053. doi: 10.1093/bjsopen/zrac053. BJS Open. 2022. PMID: 35415754 Free PMC article. No abstract available.
-
Author response to: Routine versus selective intraoperative cholangiography during cholecystectomy: a systematic review, meta-analysis, and health economic model analysis of iatrogenic bile duct injury.BJS Open. 2022 Mar 8;6(2):zrac054. doi: 10.1093/bjsopen/zrac054. BJS Open. 2022. PMID: 35415755 Free PMC article. No abstract available.
References
-
- Flum DR, Cheadle A, Prela C, Dellinger EP, Chan L. Bile duct injury during cholecystectomy and survival in Medicare beneficiaries. JAMA 2003;290:2168–2173 - PubMed
-
- GallRiks. Annual Reports. http://www.ucr.uu.se/gallriks/index.php/arsrapporter (accessed 1 January 2019)
-
- Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of biliary injury during laparoscopic cholecystectomy. J Am Coll Surg 1995;180:101–125 - PubMed
-
- Waage A, Nilsson M. Iatrogenic bile duct injury: a population-based study of 152 776 cholecystectomies in the Swedish Inpatient Registry. Arch Surg 2006;141:1207–1213 - PubMed
-
- Rystedt J, Lindell G, Montgomery A. Bile duct injuries associated with 55 134 cholecystectomies: treatment and outcome from a national perspective. World J Surg 2016;40:73–80 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
